Continuing with its magnificent efforts to help their motherland, members of American Associati9on of Physicians of Indian Origin (AAPI), the premier medical organization in the United States initiated Adopt-A-Village, a Rural Health Initiative in India during a virtual launch event on Friday, August 27, 2021. Chaired by, Dr. Satheesh Kathula, the much needed and popular program has Dr. Anupama Gotimukula, Dr. Jagan Ailinani and Dr. Ram Singh as members of the Committee.
In a rare show of support for AAPI, honorable Consul Generals of Chicago, New York, Houston, Atlanta and the Deputy CG of San Francisco participated live during the launch of this noble initiative. Ambassador of India to US, Taranjit Singh Sandhu joined the meeting with his message and lauded the numerous efforts of AAPI for India, especially during the pandemic.
Dr. Anupama Gotimukula, President, AAPI, in her welcome address, referred to the objectives of Adopt-A-Village. “A lot of efforts is being put into this initiative, “Adopt a Village” Project where AAPI in collaboration with Global TeleClinics, Inc., plans to adopt 75 villages in honor of 75 years of India’s independence,” she said. “As India celebrates her 75th anniversary Independence Day celebrations, AAPI has planned to adopt 75 villages in India spread across the states of Andhra Pradesh, Gujarat, Karnataka, Tamil Nadu and Telangana, where the rural people of India will be offered ‘Free Health Screenings in 75 Rural Villages’ for Anemia (CBC), DM (HbA1C), High Cholesterol, CKD, Malnutrition, Kidney Disease, Malnutrition, Obesity, and Hypoxemia. Results analyzed by GTC and further action recommended by their team of experts will be also, followed up. This is a small contribution from AAPI to Mother India in celebration of Azadi Ka Amrut Mahotsav.” Dr. Anupama thanked the AAPI members for their generous support for this noble work of AAPI and for sponsoring their ancestral villages and going back to their roots.
In his opening remarks, Dr. Satheesh Kathula, Chairman of AAPI’s Adopt A Village Program pointed out about the need for this noble initiative. He said, India has nearly 700,000 villages. Three out of four Indians and about 77 percent of the poor live in villages. The majority of the population has no access to safe drinking water and sanitation. The needs in these rural areas are unlimited and the scope to work are endless. “By adopting one village at a time and working with the government and NGOs, NRIs can make a difference,” he said. Dr. Kathula referred to some of the programs in place in several rural villages, including supply of Cloth mask, clean drinking water and free health care screening that has benefitted thousands of people Across India.
Dr. Ravi Kolli, President-Elect of AAPI, said, “While India has made substantial progress in health care as evidenced by the fact that life expectancy in India at birth now is 71 years as opposed to 58 years in 1990 and 41 years in 1960, there are significant gaps and divergence in health metrics in different regions in India. India, thus needs to redouble and continue its efforts and dedicate resources to tackle these perennial challenges. The post graduate training of physicians specializing in Family Medicine in every teaching institution will create a motivated and well trained family physicians to address these deficits and deliver accessible, affordable, economical and continuous preventive and primary care to rural as well urban poor populations to raise health outcomes substantially all across India,” he said.
“An individual can make a tremendous difference in the lives of many in India by adopting a village,” said Dr. Jagan Ailinani, who was instrumental in founding this noble program and set an example by adopting his own birth village in the state of Telangana in India. “A majority of the NRI’s hail from villages and would like to do their part to bring progress to villages in our state and country.”
Dr. Ram Singh said: “NRIs can adopt the village they hail from originally and make a significant contribution towards its development. There is a real will and desire on the part of governments, both at the state and the center to work with NRIs and NGOs to bring development to rural India.”
Dr. Kusum Punjabi, Chair of AAPI BOT said, “Many of these projects and programs need regular funding, and management of resources. We are grateful to dozens of AAPI members who have committed to Adopting a village in India with an ongoing commitment for investment.”
Ambassador Taranjit Singh, in his message to AAPI members, said, “As India is entering 75th year of independence, honoring men and women, who fought for the freedom, we rededicate ourselves to build an India where the dreams and aspirations of India’s 13 billion people are realized.” He urged the Diaspora community to come forward to honor INDIA by joining in the year-long celebrations.
Dr. Jayesh Shah, past President of AAPI, introduced Consul General of India in Houston, Aseem Mahajan. In his address on “Indo-US Relationship In Healthcare -Rural Health Perspective” Ambassador Mahajan told the AAPI members: “You are true the heroes and partners with us, and you make us proud, especially during the critically vital Covid times.” Urging the Diaspora to contribute towards strengthening of India’s partnership with the US, Mr. Mahajan focused on India-US partnership on various health related issues, while stressing the many healthcare initiatives by the Government of India. “AAPI can play a big role in rural health, which has been a priority for the Government of India,” he said. He thanked and appreciated the many Doctors, who are already doing similar noble initiatives, helping the rural communities have access to clean drinking water. “We can work together, collaborating and sharing of knowledge and expertise, including Medical Education,” he told AAPI.
Dr. Suresh Reddy, past President of AAPI and currently an elected Trustee of Oakbrook Village in Illinois, after introducing the Consul General of India in Chicago, Amit Kumar, announced that he is adopting his native village in the state of Telengana. In his address, Mr. Kumar spoke about “Rural Health In India, The Current Situation,” and focused on technological areas in healthcare development in the rural parts of India. “Your activities and the message to spread awareness on Covid and for providing PPEs to India are highly appreciated,” he told AAPI members, pointing to the fact that India has vaccinated over 600 million people and he hoped that India will offer vaccines to majority of India’s vast population soon.
Introduced by Dr. Sudhakar Jonnalagadda, immediate past President of India, Consul General of India in Atlanta Dr. Swati Kulkarni focused on “How AAPI and Doctors can Help India.” She said, “It’s important and laudable that you have undertaken to help India during the 75th anniversary of India’s Independence. Dr. Kulkarni shared her views on how AAPI and the government of India can collaborate in: Diplomacy for development, where “India needs overseas expertise, and you are best suited to offer,” she said, while calling upon Indian American Doctors to be part of India’s efforts to enhance the GDP. “India’s healthcare industry is growing rapidly there is more scope for growth with expanded pharma industry and medical tourism. She stressed the need for AAPI’s role in enhancing India-US political partnership, where AAPI is “a major stake holder,” she said.
Dr. Mukesh Nigam introduced Consul General of India in New York, Randhir Jaiswal. In his address on “Rural Health in India: The Challenges and Solutions” Ambassador Jaiswal said, “This noble initiative by AAPI has become more meaningful especially during the 75th anniversary of India’s Independence.” Reminding AAPI members of Modi’s call to rebuild a new India, he said, “AAPI’s initiative is even more meaningful and fits well into PM’s vision for India.” He said, ‘We applaud and thank AAPI for coming forward to help India, especially during the covid pandemic.”
Dr. Sujeeth Punnam, a renowned cardiologist introduced Deputy Consul General of India in San Francisco, Rajesh Naik. While speaking on “Rural Health, What India can learn from Developed Nations” Mr. Naik said, “AAPI has provided tremendous support as India and Indian community were struggling with the challenges of Covid. You rose to the occasion and came forward to help and support, which have been highly appreciated by the Diaspora.” During the 2nd Covid surge, AAPI stepped forward and have sent out Millions of Dollars of medical supplies to Indi, he said. While pointing to the many challenges of healthcare in rural India, Mr. Naik urged how AAPI could offer tele medical consultation in rural India, especially focusing on the preventive aspect of health in India. .
Dr. Anjana Samadder, Vice President of AAPI, said, “By adopting one village at a time and working with the government and NGOs, NRIs can make a huge difference in the lives of millions of people in India. Each project will involve a tripartite partnership between the NRI, state government and a local NGO.”
Dr. Krishan Kumar, Treasurer of AAPI pointed out, “The cost for adopting a village depends on various factors, including the population of the villages, the services that are required and what one is willing to commit to for the welfare and progress of the village one is committing to adopt.”
Dr. Lokesh Edara, chair for AAPI’s global initiative, while focusing on International medicine and how India is lagging behind in medical care, while urging the Government of India, pointed to how India needs to focus on Post Graduate Medical professionals rather than having Doctors with under graduate degree alone.
Dr. Gokula Murthy spoke about “Adopt-A-Village” by Global tele-clinics and shared with the audience as to how his firm has strived on ‘Blending medicine and technology,” while pointing to the “great opportunity to enhance the effectiveness of tele-health through awareness, education and sustainable development in all villages.”
There is no instant solution for rural India’s myriad problems. But by adopting one village at a time and working with the government and NGOs, NRIs can make a difference. Over time, an improved village could lead to an improved region, state and country.
Physicians of Indian origin are well known around the world for their compassion, passion for patient care, medical skills, research, and leadership. They have excelled in their fields of medicine, and thus have earned a name for themselves through hard work, commitment and dedication to their profession and the people they are committed to serve. Not satisfied with their own professional growth and the service they provide to their patients around the world, they are in the forefront, sharing their knowledge and expertise with others, especially those physicians and leaders in the medical field from India.
Dr. Gotimukula, urged “AAPI members to consider joining this movement and adopt a village. May be your own village of origin. AAPI will work with you in coordinating the efforts and through the support system we have in several states, will help you achieve this goal of giving back to our motherland.” AAPI members/families can sponsor a Village by emailing to: aapipresident@aapiusa.org and info@aapiusa.org. For more details, please do visit: www. aapiusa.org

 FIA’s General Secretary Richa Chand conducted the proceedings of the Annual Board Meeting for the year 2021-2022 and invited Founder President Sunil Shah for his opening remarks. Shahin his speech, outlined the successes behind the year 2021, listing the events conducted by the FIA and its team. He thanked the outgoing team for its hard work in putting together and conducting various India-centric and Charitable events during the year. He also took the opportunity to welcome new members to team FIA. In a major announcement, he declared that FIA would initiate an annual FIA Scholarship for deserving students starting from the year 2022.
FIA’s General Secretary Richa Chand conducted the proceedings of the Annual Board Meeting for the year 2021-2022 and invited Founder President Sunil Shah for his opening remarks. Shahin his speech, outlined the successes behind the year 2021, listing the events conducted by the FIA and its team. He thanked the outgoing team for its hard work in putting together and conducting various India-centric and Charitable events during the year. He also took the opportunity to welcome new members to team FIA. In a major announcement, he declared that FIA would initiate an annual FIA Scholarship for deserving students starting from the year 2022. “Though it’s too early to make any definitive statements about it, thus far it does not look like there’s a great degree of severity to it,” Fauci was quoted as saying on CNN’s ‘State of the Union on Sunday.
“Though it’s too early to make any definitive statements about it, thus far it does not look like there’s a great degree of severity to it,” Fauci was quoted as saying on CNN’s ‘State of the Union on Sunday. Some common examples of Medicare fraud include billing for services that were not provided, over billing, billing unnecessary services, misrepresenting dates of service or providers of service, and paying kickbacks for patient referrals.
Some common examples of Medicare fraud include billing for services that were not provided, over billing, billing unnecessary services, misrepresenting dates of service or providers of service, and paying kickbacks for patient referrals. Globally, more than a billion people suffer from hypertension (high blood pressure), putting them at greater risk of
Globally, more than a billion people suffer from hypertension (high blood pressure), putting them at greater risk of  The host chapter- AAPI-TN presented FFLI with a fundraised $75,000, in order to help strengthen the efforts to end human trafficking and to help continue and expand their impact in India.
The host chapter- AAPI-TN presented FFLI with a fundraised $75,000, in order to help strengthen the efforts to end human trafficking and to help continue and expand their impact in India. The underlying theme of Diwali, celebrating Light over Darkness, Victory of Good over Evil and Knowledge over Ignorance, which has caught up the attention of people all over the world, was done as the traditional lamp was lit by AAPI-TN Executive Committee, AAPI USA President Dr. Anupama Gotimukula, Congressman Jim Cooper and Grand Sponsor Dr. Bharat Sangani.
The underlying theme of Diwali, celebrating Light over Darkness, Victory of Good over Evil and Knowledge over Ignorance, which has caught up the attention of people all over the world, was done as the traditional lamp was lit by AAPI-TN Executive Committee, AAPI USA President Dr. Anupama Gotimukula, Congressman Jim Cooper and Grand Sponsor Dr. Bharat Sangani. Evolving to meet the growing needs of its members and the larger population it is called to serve, AAPI, the largest ethnic physician organization in the United states, representing over 100,000 Indian American Physicians, has grown steadily and is recognized by the authorities, local communities and mainstream media for the many noble initiatives AAPI has led, especially during the Covid pandemic, she said.
Evolving to meet the growing needs of its members and the larger population it is called to serve, AAPI, the largest ethnic physician organization in the United states, representing over 100,000 Indian American Physicians, has grown steadily and is recognized by the authorities, local communities and mainstream media for the many noble initiatives AAPI has led, especially during the Covid pandemic, she said. During the CMEs, several important topics with recent advances were well received by the AAPI fraternity. Themes for the CMEs included: ‘Cancer therapy: Advancement as we head for a cure’ by Dr. Nishitha Reddy, ‘Psychiatric sequelae of human trafficking’ by Dr. Sricharan Moturi, ‘Cardiovascular disease in South Asians- (Masala Study)’ by Dr. Ramya Suryadevara and ‘Stem cell therapy: The future of medicine’ by Dr. Sai Ram Atluri. The CME was well-attended, with active engagement between speakers and moderators (Dr. Amit Keswani, Dr.Varun Dhulipala, Dr. Biliyar, and Dr. Gunuganti. Attendees were eligible for 3 Category 1 CME hours, accredited by the Chicago Medical Society (CMS).
During the CMEs, several important topics with recent advances were well received by the AAPI fraternity. Themes for the CMEs included: ‘Cancer therapy: Advancement as we head for a cure’ by Dr. Nishitha Reddy, ‘Psychiatric sequelae of human trafficking’ by Dr. Sricharan Moturi, ‘Cardiovascular disease in South Asians- (Masala Study)’ by Dr. Ramya Suryadevara and ‘Stem cell therapy: The future of medicine’ by Dr. Sai Ram Atluri. The CME was well-attended, with active engagement between speakers and moderators (Dr. Amit Keswani, Dr.Varun Dhulipala, Dr. Biliyar, and Dr. Gunuganti. Attendees were eligible for 3 Category 1 CME hours, accredited by the Chicago Medical Society (CMS). The gala began with the Event Chair Dr. Sunil Kaza welcoming community members, family, friends, colleagues and sponsors. “We, AAPI- TN team, worked hard to stick to the mission of AAPI, for education and charity to serve humanity. We thank each and every member that attended and supported the event. Our special thanks to all our Sponsors,” said Dr. Sunil Kaza, Chair of the Gala Committee. The Grand sponsor for the event, Dr. Bharat Sangani attended the meeting personally.
The gala began with the Event Chair Dr. Sunil Kaza welcoming community members, family, friends, colleagues and sponsors. “We, AAPI- TN team, worked hard to stick to the mission of AAPI, for education and charity to serve humanity. We thank each and every member that attended and supported the event. Our special thanks to all our Sponsors,” said Dr. Sunil Kaza, Chair of the Gala Committee. The Grand sponsor for the event, Dr. Bharat Sangani attended the meeting personally. Physicians and other health professionals on the front lines of COVID-19 care have experienced so many unknowns during the pandemic. They’ve also put their own health and the well-being of their families on the line to provide care.
Physicians and other health professionals on the front lines of COVID-19 care have experienced so many unknowns during the pandemic. They’ve also put their own health and the well-being of their families on the line to provide care. AAPI’s participation at the Marathon was inspired and sponsored by the Botla Foundation, which provided a great kick start to AAPI’s wellness theme, pointed to the Six Pillars of Lifestyle Medicine: 1. Healthy Diet; 2. Being active; 3. Restorative sleep; 4. Managing stress; 5. Have social and supportive connections; and, 6. Avoiding abusive drugs and habits.
AAPI’s participation at the Marathon was inspired and sponsored by the Botla Foundation, which provided a great kick start to AAPI’s wellness theme, pointed to the Six Pillars of Lifestyle Medicine: 1. Healthy Diet; 2. Being active; 3. Restorative sleep; 4. Managing stress; 5. Have social and supportive connections; and, 6. Avoiding abusive drugs and habits. Dozens of Doctors and community leaders joined the Rock and Roll Marathon, which had attracted over 18,000 participants from around the nation, and made this an inspiring experience for all. Dr. Ravi Botla, while thanking and congratulating all the participants at the Marathon, said, “Running with you all is an amazing experience. Several friends made their personal bests today. Hope to continue to do some physical activity (running/walking/cycling) to improve our health. On behalf of all our runners yesterday and today, Botla Foundation will donate $25,000 to AAPI, irrespective of the number of participants. We should be proud of this accomplishment. Thank you Anupama and Jayesh to provide this opportunity.”
Dozens of Doctors and community leaders joined the Rock and Roll Marathon, which had attracted over 18,000 participants from around the nation, and made this an inspiring experience for all. Dr. Ravi Botla, while thanking and congratulating all the participants at the Marathon, said, “Running with you all is an amazing experience. Several friends made their personal bests today. Hope to continue to do some physical activity (running/walking/cycling) to improve our health. On behalf of all our runners yesterday and today, Botla Foundation will donate $25,000 to AAPI, irrespective of the number of participants. We should be proud of this accomplishment. Thank you Anupama and Jayesh to provide this opportunity.” “After a hiatus of 5 years from long distance running, I am thrilled to announce that I completed running the half marathon in San Antonio on a PLANT BASED DIET!” Dr. Akil Taher said. “I ran to support the American Association of Physicians of Indian origin (AAPI) under the leadership of Dr. Anupama Gotimukula ad Dr. Jayesh Shah. AAPI has done some phenomenal charity work here in the US and India. Also a big thank you to the Botla family for their inspirational support to AAPI,” he added.
“After a hiatus of 5 years from long distance running, I am thrilled to announce that I completed running the half marathon in San Antonio on a PLANT BASED DIET!” Dr. Akil Taher said. “I ran to support the American Association of Physicians of Indian origin (AAPI) under the leadership of Dr. Anupama Gotimukula ad Dr. Jayesh Shah. AAPI has done some phenomenal charity work here in the US and India. Also a big thank you to the Botla family for their inspirational support to AAPI,” he added. To run my first half-marathon with my Idol, Dr. Taher. He is a living proof of the power of ‘Whole Foods Plant Based’ Diet and Physical Exercise in not just recovering from a major surgery but healing from within for a better and stronger health than before. His presenceat the Marathon inspired us to sign up for the event and support AAPI in promoting ‘health & fitness’ in our community,” stated Dr. Bhoja R. Katipally.
To run my first half-marathon with my Idol, Dr. Taher. He is a living proof of the power of ‘Whole Foods Plant Based’ Diet and Physical Exercise in not just recovering from a major surgery but healing from within for a better and stronger health than before. His presenceat the Marathon inspired us to sign up for the event and support AAPI in promoting ‘health & fitness’ in our community,” stated Dr. Bhoja R. Katipally. The donor, Dr. Ravi Botla did his first full Marathon. There are several in the group who did their first half marathon including Dr. Jayesh Shah! We thank the Botla Foundation who inspired us! We ran with a good heart to support AAPI. Nothing is impossible if we have the motivation inside us!!” For more details on AAPI and the 40th convention, please visit:
The donor, Dr. Ravi Botla did his first full Marathon. There are several in the group who did their first half marathon including Dr. Jayesh Shah! We thank the Botla Foundation who inspired us! We ran with a good heart to support AAPI. Nothing is impossible if we have the motivation inside us!!” For more details on AAPI and the 40th convention, please visit:  The variant could lead to severe consequences in some regions, the WHO said on Monday. The head of the organisation, Dr Tedros Adhanom Ghebreyesus, renewed a call for a global push to get vaccines to poorer nations.
The variant could lead to severe consequences in some regions, the WHO said on Monday. The head of the organisation, Dr Tedros Adhanom Ghebreyesus, renewed a call for a global push to get vaccines to poorer nations. According to her, “Senior leaders from leading healthcare organizations such as pharmaceuticals, device and medical equipment manufacturers and major medical teaching institutions, hospitals and from the Ministries – Health, External/Overseas Affairs and regulatory bodies are collaborating with AAPI with the ultimate goal to provide access to high quality and affordable healthcare to all people of India.”
According to her, “Senior leaders from leading healthcare organizations such as pharmaceuticals, device and medical equipment manufacturers and major medical teaching institutions, hospitals and from the Ministries – Health, External/Overseas Affairs and regulatory bodies are collaborating with AAPI with the ultimate goal to provide access to high quality and affordable healthcare to all people of India.” Dr. Joseph Chalil, Chair of the CEO Forum said, “AAPI has made significant contributions towards addressing several issues affecting the healthcare system in India. During the GHS 2022, AAPI at the popular CEO Forum, physician leaders from the United States and India will have an opportunity to brainstorm and explore ways to focus on the theme, “Prevention is Better Than Cure” and recommend possible ways to plan and implement preventive medicine that will save resources and precious human lives.”
Dr. Joseph Chalil, Chair of the CEO Forum said, “AAPI has made significant contributions towards addressing several issues affecting the healthcare system in India. During the GHS 2022, AAPI at the popular CEO Forum, physician leaders from the United States and India will have an opportunity to brainstorm and explore ways to focus on the theme, “Prevention is Better Than Cure” and recommend possible ways to plan and implement preventive medicine that will save resources and precious human lives.” Burton said that researchers will know just how effective the vaccines are against this variant “in the next couple of weeks.” If manufacturers need to make an omicron variant-specific vaccine, it should take approximately “two to three months” to test and manufacture it, he said.
Burton said that researchers will know just how effective the vaccines are against this variant “in the next couple of weeks.” If manufacturers need to make an omicron variant-specific vaccine, it should take approximately “two to three months” to test and manufacture it, he said. “Their symptoms were so different and so mild from those I had treated before,” said Dr Coetzee, a GP for 33 years who chairs the South African Medical Association alongside running her practice.
“Their symptoms were so different and so mild from those I had treated before,” said Dr Coetzee, a GP for 33 years who chairs the South African Medical Association alongside running her practice. Late last week, the US announced a ban on flights from South Africa, Botswana, Zimbabwe, Namibia, Lesotho, Eswatini, Mozambique and Malawi. Canada, the UK and the EU and other countries have also restricted travel from southern Africa.
Late last week, the US announced a ban on flights from South Africa, Botswana, Zimbabwe, Namibia, Lesotho, Eswatini, Mozambique and Malawi. Canada, the UK and the EU and other countries have also restricted travel from southern Africa. “From the beginning, we have said that as we seek to defeat the pandemic, it is imperative that we are proactive as the virus evolves,” said Moderna CEO Stéphane Bancel. “The mutations in the Omicron variant are concerning and for several days, we have been moving as fast as possible to execute our strategy to address this variant.”
“From the beginning, we have said that as we seek to defeat the pandemic, it is imperative that we are proactive as the virus evolves,” said Moderna CEO Stéphane Bancel. “The mutations in the Omicron variant are concerning and for several days, we have been moving as fast as possible to execute our strategy to address this variant.” But “I also worry about what’s happened to our clinicians. Yes, they have been absolute heroes, but that’s coming at a cost,” said Dr. Murthy. “The question that we have to ask ourselves as a country is: Are we willing to finally step up and do something?
But “I also worry about what’s happened to our clinicians. Yes, they have been absolute heroes, but that’s coming at a cost,” said Dr. Murthy. “The question that we have to ask ourselves as a country is: Are we willing to finally step up and do something? The Ministry also issued an advisory to all ASU Drugs Manufacturers Associations seeking the manufacturers of the crude drug/extracts, sellers, ASU drug manufacturing companies, ASU drug exporters not to use Withania somnifera leaves either in crude or extract or any other form for therapeutic purposes under the ambit of ASU drugs.
The Ministry also issued an advisory to all ASU Drugs Manufacturers Associations seeking the manufacturers of the crude drug/extracts, sellers, ASU drug manufacturing companies, ASU drug exporters not to use Withania somnifera leaves either in crude or extract or any other form for therapeutic purposes under the ambit of ASU drugs. The World Health Organization says that cancer is diagnosed in more than 14 million people worldwide annually and ends up killing approximately 8.8 million. What is most shocking is that two-thirds of these deaths are in low-middle income countries where diagnosis is found to be inadequate.
The World Health Organization says that cancer is diagnosed in more than 14 million people worldwide annually and ends up killing approximately 8.8 million. What is most shocking is that two-thirds of these deaths are in low-middle income countries where diagnosis is found to be inadequate. The annual physical exam is part of the larger discussion about primary care and whether it is necessary. In the U.S., India, and other countries around the world, medicine has become the way you manage disease, not prevent it. Primary care, on the other hand, is a way to prevent disease by talking with patients about their potential health risks and giving them practical advice on how to care for their health, while considering their unique lifestyle challenges.
The annual physical exam is part of the larger discussion about primary care and whether it is necessary. In the U.S., India, and other countries around the world, medicine has become the way you manage disease, not prevent it. Primary care, on the other hand, is a way to prevent disease by talking with patients about their potential health risks and giving them practical advice on how to care for their health, while considering their unique lifestyle challenges. HHS
HHS  Overdose deaths have more than doubled since 2015, said the report, adding that it resulted from losing access to treatment, rising mental health problems and wider availability of dangerously potent street drugs.
Overdose deaths have more than doubled since 2015, said the report, adding that it resulted from losing access to treatment, rising mental health problems and wider availability of dangerously potent street drugs. Happiness can only grow and flourish in a peaceful, positive, pure and powerful mind and it will die in a mental atmosphere filled with the obstacles of negativity, anger, criticism, arrogance or depression. It is as if many of us have forgotten our original positive qualities and we have been overtaken by the negative qualities that are prevalent in our world today.
Happiness can only grow and flourish in a peaceful, positive, pure and powerful mind and it will die in a mental atmosphere filled with the obstacles of negativity, anger, criticism, arrogance or depression. It is as if many of us have forgotten our original positive qualities and we have been overtaken by the negative qualities that are prevalent in our world today. “Vaccination is just one tool. It’s not a silver bullet,” she told DW. “Vaccines are very effective against protecting against severe disease…But vaccines are not 100% effective against infection.”
“Vaccination is just one tool. It’s not a silver bullet,” she told DW. “Vaccines are very effective against protecting against severe disease…But vaccines are not 100% effective against infection.” “As the President, one of my main goal is to revitalize local Chapters that are the backbone for the national organization; help make the local Chapters financially viable as funds have dwindled due to pharma support; and to bring in younger physicians into the fold,” the young and dynamic President told a select group of audience who had come to cheer him and the new executive committee.
“As the President, one of my main goal is to revitalize local Chapters that are the backbone for the national organization; help make the local Chapters financially viable as funds have dwindled due to pharma support; and to bring in younger physicians into the fold,” the young and dynamic President told a select group of audience who had come to cheer him and the new executive committee. “I would also like to thank all the leaders of IAMA, especially Drs, Vemuri Murthy, Hanumadass, Rohit Vasa, Satya Ahuja, Shastri Swaminathan, Khandelwal, Arvind Goyal, Annita John, Utpal Parikh, Sukanya Reddy and several others.” He had a special note for Dr. Lalmalani. “I would like to thank my spiritual guru and political mentor, our Mayor of Oak Brook Dr. Lalmalani.”
“I would also like to thank all the leaders of IAMA, especially Drs, Vemuri Murthy, Hanumadass, Rohit Vasa, Satya Ahuja, Shastri Swaminathan, Khandelwal, Arvind Goyal, Annita John, Utpal Parikh, Sukanya Reddy and several others.” He had a special note for Dr. Lalmalani. “I would like to thank my spiritual guru and political mentor, our Mayor of Oak Brook Dr. Lalmalani.” Author of many international medical journal articles, Dr. Reddy has traveled extensively, giving specialty lectures on the complex procedures that he does. Active in teaching and mentoring many medical students and residents, Dr. Reddy has received numerous teaching and mentoring awards. To his credit, he is a four-time recipient of “Faculty award for excellence in teaching” awarded by the Harvard Medical Students and Residents.
Author of many international medical journal articles, Dr. Reddy has traveled extensively, giving specialty lectures on the complex procedures that he does. Active in teaching and mentoring many medical students and residents, Dr. Reddy has received numerous teaching and mentoring awards. To his credit, he is a four-time recipient of “Faculty award for excellence in teaching” awarded by the Harvard Medical Students and Residents. In the summer of 2019, Dr. Reddy organized The Global Health Summit in Hyderabad, an educational event with numerous workshops. Vice President of India, Sri Venkaiah Naidu, Union Minster of Health, Dr. Harshvardhan, both addressed the highly successful Global Health Summit. In October of 2019, he played a key role along with the Indian Resuscitation Council to train almost 500,000 lay people in Cardio-Pulmonary Resuscitation in India.
In the summer of 2019, Dr. Reddy organized The Global Health Summit in Hyderabad, an educational event with numerous workshops. Vice President of India, Sri Venkaiah Naidu, Union Minster of Health, Dr. Harshvardhan, both addressed the highly successful Global Health Summit. In October of 2019, he played a key role along with the Indian Resuscitation Council to train almost 500,000 lay people in Cardio-Pulmonary Resuscitation in India. His leadership and foresight were deeply appreciated as AAPI became the first major organization to call for universal masking. In this regard, AAPI provided free masks to thousands of health care workers. AAPI members have honored more than 10,000 nurses in over 100 hospitals across more than 40 states by sponsoring lunches for them during the Nurses Week. He was instrumental in organizing the Obesity prevention programs in all continenets, sharing medical knowledge globally, team-building activities such as the Share-A-Blanket program, medical education programs such as CPR training, morale building programs like mentoring a future medical students, and India heritage programs like Independence Day celebrations.
His leadership and foresight were deeply appreciated as AAPI became the first major organization to call for universal masking. In this regard, AAPI provided free masks to thousands of health care workers. AAPI members have honored more than 10,000 nurses in over 100 hospitals across more than 40 states by sponsoring lunches for them during the Nurses Week. He was instrumental in organizing the Obesity prevention programs in all continenets, sharing medical knowledge globally, team-building activities such as the Share-A-Blanket program, medical education programs such as CPR training, morale building programs like mentoring a future medical students, and India heritage programs like Independence Day celebrations. IAMA-IL is a non-profit organization comprised of Illinois physicians, fellows, residents, and medical students of Indian origin who are committed to professional excellence and quality patient care. IAMA-IL offers many opportunities for your organization to begin and grow a connection with our members and the communities we serve. We like to partner with organizations and people that strive for similar goals including a commitment to excellence, education, research and serving the community.
IAMA-IL is a non-profit organization comprised of Illinois physicians, fellows, residents, and medical students of Indian origin who are committed to professional excellence and quality patient care. IAMA-IL offers many opportunities for your organization to begin and grow a connection with our members and the communities we serve. We like to partner with organizations and people that strive for similar goals including a commitment to excellence, education, research and serving the community. In this regard, he highlighted some data points from the WHO Global Report on Traditional and Complementary Medicine 2019 – number of countries with national policy on traditional and complementary medicine has increased from 25 in 1998 to 98 in 2019 and countries with health insurance cover for traditional and complementary medicine has increased from 37 in 2012 to 45 in 2018. Consul General underlined the vast network of scientific studies being undertaken on Ayurveda in universities in the United States and in research ecosystems across the world including in India.
In this regard, he highlighted some data points from the WHO Global Report on Traditional and Complementary Medicine 2019 – number of countries with national policy on traditional and complementary medicine has increased from 25 in 1998 to 98 in 2019 and countries with health insurance cover for traditional and complementary medicine has increased from 37 in 2012 to 45 in 2018. Consul General underlined the vast network of scientific studies being undertaken on Ayurveda in universities in the United States and in research ecosystems across the world including in India. CNN chief medical correspondent Sanjay Gupta, MD, offers an accessible, data-packed answer to our biggest questions about Covid-19: What have we learned about this pandemic and how can we prepare for—or prevent—the next one?
CNN chief medical correspondent Sanjay Gupta, MD, offers an accessible, data-packed answer to our biggest questions about Covid-19: What have we learned about this pandemic and how can we prepare for—or prevent—the next one? Gupta argues that we need to prepare for a new era where pandemics will be more frequent, and possibly even more deadly. As the doctor who’s been holding America’s hand through the crisis with compassion, clarity, and well-earned wisdom, he gives you the unvarnished story behind the pandemic, including insights about the novel virus’s behavior, and offers practical tools to ready ourselves for what lies ahead. He answers critical questions: Can we stamp out the virus for good (and if not, how do we live with it)? Should we put our parents in a nursing home? Where should we live? What should we stockpile? What should we know before taking a trip? Does it make sense to spend more on health insurance to deal with any long-term effects? How do you decide when it’s safe to go to a public pool or schedule elective surgery? What should Covid survivors know about protecting their future health? What if you become a long-hauler with chronic health challenges stemming?
Gupta argues that we need to prepare for a new era where pandemics will be more frequent, and possibly even more deadly. As the doctor who’s been holding America’s hand through the crisis with compassion, clarity, and well-earned wisdom, he gives you the unvarnished story behind the pandemic, including insights about the novel virus’s behavior, and offers practical tools to ready ourselves for what lies ahead. He answers critical questions: Can we stamp out the virus for good (and if not, how do we live with it)? Should we put our parents in a nursing home? Where should we live? What should we stockpile? What should we know before taking a trip? Does it make sense to spend more on health insurance to deal with any long-term effects? How do you decide when it’s safe to go to a public pool or schedule elective surgery? What should Covid survivors know about protecting their future health? What if you become a long-hauler with chronic health challenges stemming? “We invite you to the AAPI 40th Annual Convention in the beautiful city of San Antonio, Texas,” Dr. Jayesh Shah, past President of AAPI and Chair of AAPI Convention 2022 said. Welcoming the delegates to his “Home city of San Antonio,” which is hosting the 2nd national convention, Dr. Shah said, “We have convened a fantastic group of people to meet the needs of the 2022 convention and are very excited about this year. Please reach out to any one of the representatives from the San Antonio team with questions or comments.”
“We invite you to the AAPI 40th Annual Convention in the beautiful city of San Antonio, Texas,” Dr. Jayesh Shah, past President of AAPI and Chair of AAPI Convention 2022 said. Welcoming the delegates to his “Home city of San Antonio,” which is hosting the 2nd national convention, Dr. Shah said, “We have convened a fantastic group of people to meet the needs of the 2022 convention and are very excited about this year. Please reach out to any one of the representatives from the San Antonio team with questions or comments.” “Our physician members have worked very hard during the covid 19 pandemic as the 2022 convention is a perfect time to heal the healers with a special focus on wellness,” said Dr. Jayesh Shah. Accordingly, some of the major themes at the convention include: Yoga and Meditation practices, Welcome kit with books & self-care supplies, A Personal Reflexology Session, Take home wellness routine, Ailment based yoga therapy sessions, Workshop on Spiritual well-being, Book talk with Yoga Gurus, including on the science of Yoga & Lifestyle medicine, as well as a unique opportunity to visit first of its kind in San Antonio, Aum Ashram as part of the Wellness session.
“Our physician members have worked very hard during the covid 19 pandemic as the 2022 convention is a perfect time to heal the healers with a special focus on wellness,” said Dr. Jayesh Shah. Accordingly, some of the major themes at the convention include: Yoga and Meditation practices, Welcome kit with books & self-care supplies, A Personal Reflexology Session, Take home wellness routine, Ailment based yoga therapy sessions, Workshop on Spiritual well-being, Book talk with Yoga Gurus, including on the science of Yoga & Lifestyle medicine, as well as a unique opportunity to visit first of its kind in San Antonio, Aum Ashram as part of the Wellness session. Metkar’s identification as the “first named inventor” is in the document filed by Moderna to dispute the U.S. government’s National Institutes of Health assertion that its scientists should also be credited as inventors of the vaccine, which was developed in collaboration with it and with $1.53 billion provided by the administration of former President Donald Trump under the Operation Warp Speed program to quickly produce vaccines.
Metkar’s identification as the “first named inventor” is in the document filed by Moderna to dispute the U.S. government’s National Institutes of Health assertion that its scientists should also be credited as inventors of the vaccine, which was developed in collaboration with it and with $1.53 billion provided by the administration of former President Donald Trump under the Operation Warp Speed program to quickly produce vaccines. Like Pfizer-BioNTech’s adult vaccine, the pediatric version is meant to be given in two doses, spaced three weeks apart. Each dose, however, is smaller than that given to adults.
Like Pfizer-BioNTech’s adult vaccine, the pediatric version is meant to be given in two doses, spaced three weeks apart. Each dose, however, is smaller than that given to adults. Two studies show one of four flu viruses that infect humans each year hasn’t been detected anywhere in the world since April 2020.
Two studies show one of four flu viruses that infect humans each year hasn’t been detected anywhere in the world since April 2020. The Covid pandemic has impacted all aspects of human life as never been before. The past two years have been challenging to everyone, particularly those are assigned with the responsibility of caring for the sick, especially as hundreds of Millions were affected by the big pandemic. Over 115,000 health care workers died from Covid-19 from January 2020 to May of this year, according to a new World Health Organization estimate.
The Covid pandemic has impacted all aspects of human life as never been before. The past two years have been challenging to everyone, particularly those are assigned with the responsibility of caring for the sick, especially as hundreds of Millions were affected by the big pandemic. Over 115,000 health care workers died from Covid-19 from January 2020 to May of this year, according to a new World Health Organization estimate. Accordingly, some of the major themes at the convention include: Yoga and Meditation practices, Welcome kit with books & self-care supplies, A Personal Reflexology Session, Take home wellness routine, Ailment based yoga therapy sessions, Workshop on Spiritual well-being, Book talk with Yoga Gurus, including on the science of Yoga & Lifestyle medicine, as well as an unique opportunity to visit first of its kind in San Antonio, Aum Ashram as part of the Wellness session.
Accordingly, some of the major themes at the convention include: Yoga and Meditation practices, Welcome kit with books & self-care supplies, A Personal Reflexology Session, Take home wellness routine, Ailment based yoga therapy sessions, Workshop on Spiritual well-being, Book talk with Yoga Gurus, including on the science of Yoga & Lifestyle medicine, as well as an unique opportunity to visit first of its kind in San Antonio, Aum Ashram as part of the Wellness session. The FDA panel accepted
The FDA panel accepted  The TAG — which is an independent advisory group that recommends to WHO on whether a Covid-19 vaccine fulfils criteria for EUL or not — will meet next on November 3.
The TAG — which is an independent advisory group that recommends to WHO on whether a Covid-19 vaccine fulfils criteria for EUL or not — will meet next on November 3. Building on earlier work with Tiffany Ford from May 2020, “
Building on earlier work with Tiffany Ford from May 2020, “ We recently learned that there are certain
We recently learned that there are certain  PM Narendra Modi tweeted: “The journey from anxiety to assurance has happened and our nation has emerged stronger, thanks to the world’s largest vaccination drive.”
PM Narendra Modi tweeted: “The journey from anxiety to assurance has happened and our nation has emerged stronger, thanks to the world’s largest vaccination drive.” Certain people who received Pfizer vaccinations months ago already are eligible for a booster and now the Centers for Disease Control and Prevention says specific Moderna and Johnson & Johnson recipients qualify, too. And in a bigger change, the agency is allowing the flexibility of “mixing and matching” that extra dose regardless of which type people received first.
Certain people who received Pfizer vaccinations months ago already are eligible for a booster and now the Centers for Disease Control and Prevention says specific Moderna and Johnson & Johnson recipients qualify, too. And in a bigger change, the agency is allowing the flexibility of “mixing and matching” that extra dose regardless of which type people received first. The hearings will take place one month before the Supreme Court is set to hear arguments in another pivotal abortion case, Dobbs v. Jackson Women’s Health, which directly challenges the abortion-rights precedent established in 1973 under Roe v. Wade. The court announced on Friday its decision to hear arguments over whether the Biden administration had the right to sue to end enforcement of the law, Sotomayor indicated that she
The hearings will take place one month before the Supreme Court is set to hear arguments in another pivotal abortion case, Dobbs v. Jackson Women’s Health, which directly challenges the abortion-rights precedent established in 1973 under Roe v. Wade. The court announced on Friday its decision to hear arguments over whether the Biden administration had the right to sue to end enforcement of the law, Sotomayor indicated that she  Led by Professor Shulamit Levenberg, Ph.D. student Rita Beckerman from the Stem Cell and Tissue Engineering Laboratory in the Technion’s Faculty of Biomedical Engineering presents a novel treatment approach, using an autograft of muscle cells engineered to take in sugar at increased rates. Mice treated in this manner displayed normal blood sugar levels for months after a single procedure. The group’s findings were recently published in
Led by Professor Shulamit Levenberg, Ph.D. student Rita Beckerman from the Stem Cell and Tissue Engineering Laboratory in the Technion’s Faculty of Biomedical Engineering presents a novel treatment approach, using an autograft of muscle cells engineered to take in sugar at increased rates. Mice treated in this manner displayed normal blood sugar levels for months after a single procedure. The group’s findings were recently published in  “Data from 119 countries suggest that on average, two in five healthcare workers globally are fully vaccinated,” Dr Tedros said. “But of course, that average masks huge differences across regions and economic groupings.” Fewer than one in 10 healthcare workers were fully vaccinated in Africa, he said, compared with eight in 10 in high-income countries. A failure to provide poorer countries with enough vaccines was highlighted earlier by Dr Bruce Aylward, a senior leader at the WHO, who said it meant the Covid crisis could “easily drag on deep into 2022”.
“Data from 119 countries suggest that on average, two in five healthcare workers globally are fully vaccinated,” Dr Tedros said. “But of course, that average masks huge differences across regions and economic groupings.” Fewer than one in 10 healthcare workers were fully vaccinated in Africa, he said, compared with eight in 10 in high-income countries. A failure to provide poorer countries with enough vaccines was highlighted earlier by Dr Bruce Aylward, a senior leader at the WHO, who said it meant the Covid crisis could “easily drag on deep into 2022”. Dr. V.K. Raju, who was born in Rajahmundry, AP, India, is a Clinical Professor of Ophthalmology at West Virginia University, Fellow of the Royal College of Surgeons, Fellow of the American College of Surgeons, Director of the International Ocular Surface Society, Director of the Ocular Surface Research and Education Foundation, Chairman of Goutami Eye Institute in Rajahmundry and is the President and Founder of the Eye Foundation of America, a non-profit organization dedicated to realizing a world without childhood blindness.
Dr. V.K. Raju, who was born in Rajahmundry, AP, India, is a Clinical Professor of Ophthalmology at West Virginia University, Fellow of the Royal College of Surgeons, Fellow of the American College of Surgeons, Director of the International Ocular Surface Society, Director of the Ocular Surface Research and Education Foundation, Chairman of Goutami Eye Institute in Rajahmundry and is the President and Founder of the Eye Foundation of America, a non-profit organization dedicated to realizing a world without childhood blindness. Dr. Raju expressed gratitude to all the Board members of the Foundation in UK, particularly, Ashwini Misro, Radhika Misro, and Raj Koppada for their enthusiasm and generosity in helping realize the mission of the Eye Foundation in preventing and treating childhood blindness and beyond in Uzbekistan.
Dr. Raju expressed gratitude to all the Board members of the Foundation in UK, particularly, Ashwini Misro, Radhika Misro, and Raj Koppada for their enthusiasm and generosity in helping realize the mission of the Eye Foundation in preventing and treating childhood blindness and beyond in Uzbekistan. In this context, as part of an ongoing awareness and education campaign about high risk heart disease in South Asians, American Association of Physicians of Indian Origin (AAPI) the largest ethnic medical organization in the United States presented two eminent speakers and experts, Dr. Enas Enas and Dr. Amit Kera, discussing ways to create awareness on Heart Disease Among South Asians during a webinar on Saturday, October 16th, 2021.
In this context, as part of an ongoing awareness and education campaign about high risk heart disease in South Asians, American Association of Physicians of Indian Origin (AAPI) the largest ethnic medical organization in the United States presented two eminent speakers and experts, Dr. Enas Enas and Dr. Amit Kera, discussing ways to create awareness on Heart Disease Among South Asians during a webinar on Saturday, October 16th, 2021. Dr. Enas referred to several research/studies around the world, showing high prevalence of CAD among Indians. “Indians have a big problem with premature heart disease,” Dr. Enas said and pointed out that 185,000 people of South Asian origin die of heart disease per year as against 15,000 Whites die of the same health issue. While referring to Mitigating Risk Factors, Dr. Enas recommended Indians to follow the American Heart Association developed Life Simple 7 with additional requirement for exercise and maintaining sugar level below 140.
Dr. Enas referred to several research/studies around the world, showing high prevalence of CAD among Indians. “Indians have a big problem with premature heart disease,” Dr. Enas said and pointed out that 185,000 people of South Asian origin die of heart disease per year as against 15,000 Whites die of the same health issue. While referring to Mitigating Risk Factors, Dr. Enas recommended Indians to follow the American Heart Association developed Life Simple 7 with additional requirement for exercise and maintaining sugar level below 140. Dr. Amit Kera, a new rising star in Preventive Cardiology, built on that argument and presented genomic data to fill the gap and also pointed out that usual risk scoring has been done on Caucasians and cannot be extrapolated to south Asians. He advocated for the need for our own data base and especially genomic data to go beyond coronary calcium score and use “ Polygenic score,” which can predict even more accurately the risk of heart disease individually what he calls “Precision Medicine,” a futuristic concept, which he is working on as Associate Director at prestigious Broad institute affiliated with MIT and Harvard. Pointing to international studies that point to prevalence of Cardiovascular diseases high among South Asians, he said, Diabetes is diagnosed four times more among the Asians in comparison with Europeans.
Dr. Amit Kera, a new rising star in Preventive Cardiology, built on that argument and presented genomic data to fill the gap and also pointed out that usual risk scoring has been done on Caucasians and cannot be extrapolated to south Asians. He advocated for the need for our own data base and especially genomic data to go beyond coronary calcium score and use “ Polygenic score,” which can predict even more accurately the risk of heart disease individually what he calls “Precision Medicine,” a futuristic concept, which he is working on as Associate Director at prestigious Broad institute affiliated with MIT and Harvard. Pointing to international studies that point to prevalence of Cardiovascular diseases high among South Asians, he said, Diabetes is diagnosed four times more among the Asians in comparison with Europeans. Binghamton University Professor of Political Science Olga Shvetsova
Binghamton University Professor of Political Science Olga Shvetsova The COVID-19 vaccine made by
The COVID-19 vaccine made by  The disease is the most prevalent form of cancer globally and has become a major problem in India, where breast cancer accounts for 25% to 31% of all cancers.
The disease is the most prevalent form of cancer globally and has become a major problem in India, where breast cancer accounts for 25% to 31% of all cancers. The CDC published data Oct. 15 that breaks down the rate of COVID-19 cases and deaths by vaccination status and vaccine type. The rates are based on data from 16 public health departments — representing about 30 percent of the U.S. population — and cover April through the end of August.
The CDC published data Oct. 15 that breaks down the rate of COVID-19 cases and deaths by vaccination status and vaccine type. The rates are based on data from 16 public health departments — representing about 30 percent of the U.S. population — and cover April through the end of August.  The $20 copay was well worth it for the 26-year-old ad salesman, whose girlfriend also routinely relies on telehealth to see her nutritionist. “It’s a very easy way to get an expert opinion without having to necessarily leave your apartment,” fill out forms or spend idle time in waiting rooms, Freyre says. “We all know what going to the doctor can be like.”But now, Freyre has a sore knee — and he’s not content to to visit his doctor by phone or Zoom. “That’s something that I will 100% want handled in person.”
The $20 copay was well worth it for the 26-year-old ad salesman, whose girlfriend also routinely relies on telehealth to see her nutritionist. “It’s a very easy way to get an expert opinion without having to necessarily leave your apartment,” fill out forms or spend idle time in waiting rooms, Freyre says. “We all know what going to the doctor can be like.”But now, Freyre has a sore knee — and he’s not content to to visit his doctor by phone or Zoom. “That’s something that I will 100% want handled in person.” “If you boost people who have originally received J&J with either Moderna or Pfizer, the level of antibodies that you induce in them is much higher than if you boost them with the original J&J,” Fauci told reporters during a television interview.
“If you boost people who have originally received J&J with either Moderna or Pfizer, the level of antibodies that you induce in them is much higher than if you boost them with the original J&J,” Fauci told reporters during a television interview. A highly anticipated study of “mixing and matching” Covid-19 vaccines found the approach to be safe and effective, although the Moderna and Pfizer-BioNTech vaccines were found to spark stronger immune system responses than Johnson & Johnson’s vaccine. “Mixing and matching” refers to giving a booster dose of a vaccine different from the vaccine type that was used for the initial vaccination series.
A highly anticipated study of “mixing and matching” Covid-19 vaccines found the approach to be safe and effective, although the Moderna and Pfizer-BioNTech vaccines were found to spark stronger immune system responses than Johnson & Johnson’s vaccine. “Mixing and matching” refers to giving a booster dose of a vaccine different from the vaccine type that was used for the initial vaccination series. ICC’s 18th annual gala was held virtually for the second time, in keeping with Covid-19 safety protocols, which discourage gatherings of large groups indoors. A friendly-but-competitive live auction, followed by a lively pledge drive, quickly raised more than $257,000 to support the community center, a second home to many Indian American seniors and youth. “J&J, BioNTech, and Moderna had never created vaccines before. But everyone saw the public health crisis that was happening — as 10,000 people died each day — and wanted to help,” said Mammen, who was interviewed at the gala by Divya Ganesan, a Stanford University freshman, and co-founder of Real Talk Ed.
ICC’s 18th annual gala was held virtually for the second time, in keeping with Covid-19 safety protocols, which discourage gatherings of large groups indoors. A friendly-but-competitive live auction, followed by a lively pledge drive, quickly raised more than $257,000 to support the community center, a second home to many Indian American seniors and youth. “J&J, BioNTech, and Moderna had never created vaccines before. But everyone saw the public health crisis that was happening — as 10,000 people died each day — and wanted to help,” said Mammen, who was interviewed at the gala by Divya Ganesan, a Stanford University freshman, and co-founder of Real Talk Ed. The WHO said on Wednesday its recommendation is based on results from more than 2.3 million doses of the vaccine that have been administered to more than 800,000 children in pilot countries Ghana, Kenya and Malawi since 2019, Xinhua news agency reported.
The WHO said on Wednesday its recommendation is based on results from more than 2.3 million doses of the vaccine that have been administered to more than 800,000 children in pilot countries Ghana, Kenya and Malawi since 2019, Xinhua news agency reported. Incorporating cutting-edge science on nutrients, food ingredients, processing characteristics, phytochemicals, and additives (existing systems focus largely on just a few nutrients); and Objectively scoring all foods, beverages, and even mixed dishes and meals using one consistent score (existing systems subjectively group and score foods differently). “Once you get beyond ‘eat your veggies, avoid soda,’ the public is pretty confused about how to identify healthier choices in the grocery store, cafeteria, and restaurant,” said the study’s lead and corresponding author,
Incorporating cutting-edge science on nutrients, food ingredients, processing characteristics, phytochemicals, and additives (existing systems focus largely on just a few nutrients); and Objectively scoring all foods, beverages, and even mixed dishes and meals using one consistent score (existing systems subjectively group and score foods differently). “Once you get beyond ‘eat your veggies, avoid soda,’ the public is pretty confused about how to identify healthier choices in the grocery store, cafeteria, and restaurant,” said the study’s lead and corresponding author,  “Harnessing the power of Indian Doctors worldwide, the AAPI Global Healthcare Summit platform has evolved with the support of prominent global and Indian medical associations,” says Dr. Anupama Gotimukula, President of AAPI. “The theme for the Summit this year is, ‘Prevention Is Better Than Cure Through Technology, Telemedicine & Transformation’ and we want to coordinate and collaborate all our resources towards helping India emerge stronger and healthier.”
“Harnessing the power of Indian Doctors worldwide, the AAPI Global Healthcare Summit platform has evolved with the support of prominent global and Indian medical associations,” says Dr. Anupama Gotimukula, President of AAPI. “The theme for the Summit this year is, ‘Prevention Is Better Than Cure Through Technology, Telemedicine & Transformation’ and we want to coordinate and collaborate all our resources towards helping India emerge stronger and healthier.” “Physicians and delegates from different parts of the world will come together, facilitating exchange of knowledge, cutting edge technology and best practices in protecting and promoting healthcare,” Dr. Udaya Shivangi, Chair of AAPI GHS USA 2021 says. “In addition to continuing the ongoing projects commenced by past AAPI leaders, GHS will have new initiatives and innovative ideas. The GHS 2022 will focus on envisioning future digital health solutions, and preventive strategies with state of the art CMEs and Symposiums with information on current and emerging issues and trends in healthcare.”While elaborating on the themes and areas that are going to be covered during the Summit, Dr. Kusum Punjabi, Chair of AAPI BOT, says, “In our efforts to realize the core mission of AAPI, which is to share the best from leading experts from around the world, to collaborate on clinical challenges, research and development, philanthropy, policy and standards formulation, the Summit in Hyderabad will have clinical tracks that are of vital to healthcare in India.”
“Physicians and delegates from different parts of the world will come together, facilitating exchange of knowledge, cutting edge technology and best practices in protecting and promoting healthcare,” Dr. Udaya Shivangi, Chair of AAPI GHS USA 2021 says. “In addition to continuing the ongoing projects commenced by past AAPI leaders, GHS will have new initiatives and innovative ideas. The GHS 2022 will focus on envisioning future digital health solutions, and preventive strategies with state of the art CMEs and Symposiums with information on current and emerging issues and trends in healthcare.”While elaborating on the themes and areas that are going to be covered during the Summit, Dr. Kusum Punjabi, Chair of AAPI BOT, says, “In our efforts to realize the core mission of AAPI, which is to share the best from leading experts from around the world, to collaborate on clinical challenges, research and development, philanthropy, policy and standards formulation, the Summit in Hyderabad will have clinical tracks that are of vital to healthcare in India.” These findings,
These findings,  Health experts say the fourth wave of the pandemic has peaked overall in the U.S., particularly in the Deep South, where hospitals were stretched to the limit weeks ago. But many Northern states are still struggling with rising cases, and what’s ahead for winter is far less clear. Unknowns include how flu season may strain already depleted hospital staffs and whether those who have refused to get vaccinated will change their minds.
Health experts say the fourth wave of the pandemic has peaked overall in the U.S., particularly in the Deep South, where hospitals were stretched to the limit weeks ago. But many Northern states are still struggling with rising cases, and what’s ahead for winter is far less clear. Unknowns include how flu season may strain already depleted hospital staffs and whether those who have refused to get vaccinated will change their minds. It found that about 36% of Covid patients still reported disease symptoms three and six months after diagnosis. Most previous studies estimated the so-called long-haul Covid to afflict 10% to 30% of patients. The researchers also found that of those who had long COVID three to six months after diagnosis, roughly 40% had no record of such symptoms in the prior three months.
It found that about 36% of Covid patients still reported disease symptoms three and six months after diagnosis. Most previous studies estimated the so-called long-haul Covid to afflict 10% to 30% of patients. The researchers also found that of those who had long COVID three to six months after diagnosis, roughly 40% had no record of such symptoms in the prior three months. What is the unique health ID, and how does one get it?
What is the unique health ID, and how does one get it? In the course of the COVID-19 pandemic, thousands of variants have been identified, four of which are considered “
In the course of the COVID-19 pandemic, thousands of variants have been identified, four of which are considered “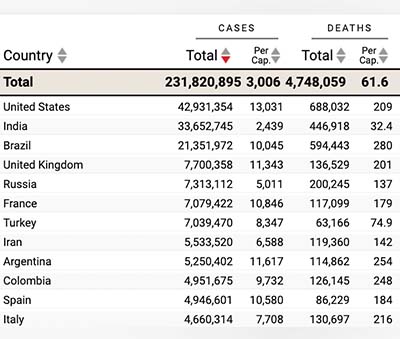 Coronaviruses more prone to mutations than other germs
Coronaviruses more prone to mutations than other germs The Governor of Sikkim, Ganga Prasad, praised the foundation initiative and congratulated all the awardees. He launched the stickers, “I Salute Doctors”, in the presence of all the dignitaries. He said Nisha foundation is working towards a wonderful mission for betterment of society. Kulstey said Nisha foundation initiative is great and he applaud this program and appreciated Nisha foundation for working in 173 countries in association of world Organization of peace for child education, sports and salutation evening in name of frontliners During his speech he said it’s important to do this kind of programs to uplift human consciousness and he expressed his concern for farmers.
The Governor of Sikkim, Ganga Prasad, praised the foundation initiative and congratulated all the awardees. He launched the stickers, “I Salute Doctors”, in the presence of all the dignitaries. He said Nisha foundation is working towards a wonderful mission for betterment of society. Kulstey said Nisha foundation initiative is great and he applaud this program and appreciated Nisha foundation for working in 173 countries in association of world Organization of peace for child education, sports and salutation evening in name of frontliners During his speech he said it’s important to do this kind of programs to uplift human consciousness and he expressed his concern for farmers. Across the world, the 1918-19 influenza pandemic killed 50 million victims globally at a time when the world had one-quarter the population it does now. Global deaths from COVID-19 now stand at more than 4.6 million. For now, the pandemic still has the United States and other parts of the world firmly in its jaws. While the delta-fueled surge in infections may have peaked, U.S. deaths are running at over 1,900 a day on average, the highest level since early March, and the country’s overall toll topped 675,000 on Monday, September 20th, according to the count kept by Johns Hopkins University, though the real number is believed to be higher.
Across the world, the 1918-19 influenza pandemic killed 50 million victims globally at a time when the world had one-quarter the population it does now. Global deaths from COVID-19 now stand at more than 4.6 million. For now, the pandemic still has the United States and other parts of the world firmly in its jaws. While the delta-fueled surge in infections may have peaked, U.S. deaths are running at over 1,900 a day on average, the highest level since early March, and the country’s overall toll topped 675,000 on Monday, September 20th, according to the count kept by Johns Hopkins University, though the real number is believed to be higher. The ebbing of COVID-19 could happen if the virus progressively weakens as it mutates and more and more humans’ immune systems learn to attack it. Vaccination and surviving infection are the main ways the immune system improves. Breast-fed infants also gain some immunity from their mothers. Under that optimistic scenario, schoolchildren would get mild illness that trains their immune systems. As they grow up, the children would carry the immune response memory, so that when they are old and vulnerable, the coronavirus would be no more dangerous than cold viruses.
The ebbing of COVID-19 could happen if the virus progressively weakens as it mutates and more and more humans’ immune systems learn to attack it. Vaccination and surviving infection are the main ways the immune system improves. Breast-fed infants also gain some immunity from their mothers. Under that optimistic scenario, schoolchildren would get mild illness that trains their immune systems. As they grow up, the children would carry the immune response memory, so that when they are old and vulnerable, the coronavirus would be no more dangerous than cold viruses. The US, where Covid-19 is now officially the deadliest epidemic since the Spanish Flu of 1918 with over 675,000 deaths, has also seen a rather high number of infections among children. For the week ended September 9, new infections among children totaled 243,000 and constitute 30% of all new infections in the country. Up until January this year, children made up just 15% of new Covid-19 infections in the US.
The US, where Covid-19 is now officially the deadliest epidemic since the Spanish Flu of 1918 with over 675,000 deaths, has also seen a rather high number of infections among children. For the week ended September 9, new infections among children totaled 243,000 and constitute 30% of all new infections in the country. Up until January this year, children made up just 15% of new Covid-19 infections in the US. Although the result wasn’t what Pfizer-BioNTech expected, Kathrin Jansen, senior vice president and head of vaccine research and development at Pfizer, said in a statement that “these data, and the larger body of scientific evidence presented at the meeting, underscore our belief that boosters will be a critical tool in the ongoing effort to control the spread of this virus. We thank the committee for their thoughtful review of the data and will work with the FDA following today’s meeting to address the committee’s questions, as we continue to believe in the benefits of a booster dose for a broader population.”
Although the result wasn’t what Pfizer-BioNTech expected, Kathrin Jansen, senior vice president and head of vaccine research and development at Pfizer, said in a statement that “these data, and the larger body of scientific evidence presented at the meeting, underscore our belief that boosters will be a critical tool in the ongoing effort to control the spread of this virus. We thank the committee for their thoughtful review of the data and will work with the FDA following today’s meeting to address the committee’s questions, as we continue to believe in the benefits of a booster dose for a broader population.” Dr. Anupama Gotimukula, President of AAPI while congratulating the Editorial Team of JAAPI said, “This is the fruit of our teamwork and it’s a good opportunity for the members of AAPI to contribute scientific articles, and make it better as we move on. JAAPI is a peer-reviewed medical and health journal published by the AAPI. In line with the vision and mission of AAPI, JAAPI is dedicated to facilitate physicians to excel in patient care, teaching and research, and thus pursue their aspirations in professional and community affairs. JAAPI is open to contributions from physicians and scientists of all backgrounds and from all over the world.” In his introductory note, the Founding Editor-in-Chief of the peer-reviewed JAAPI, Dr. Bellamkonda K. Kishore, who is an outstanding academician, innovator, and entrepreneur, writes, “ We are pleased to present you the Summer issue of peer-reviewed JAAPI. It is made possible with the unconditional support of AAPI President Dr. Anupama Gotimukula and the Executive Committee Members, the relentless work of Members of the JAAPI Editorial Board, Editorial Advisors, and Reviewers as well as Ms. Vijaya Kodali, the Chief Operations Officer of AAPI.”
Dr. Anupama Gotimukula, President of AAPI while congratulating the Editorial Team of JAAPI said, “This is the fruit of our teamwork and it’s a good opportunity for the members of AAPI to contribute scientific articles, and make it better as we move on. JAAPI is a peer-reviewed medical and health journal published by the AAPI. In line with the vision and mission of AAPI, JAAPI is dedicated to facilitate physicians to excel in patient care, teaching and research, and thus pursue their aspirations in professional and community affairs. JAAPI is open to contributions from physicians and scientists of all backgrounds and from all over the world.” In his introductory note, the Founding Editor-in-Chief of the peer-reviewed JAAPI, Dr. Bellamkonda K. Kishore, who is an outstanding academician, innovator, and entrepreneur, writes, “ We are pleased to present you the Summer issue of peer-reviewed JAAPI. It is made possible with the unconditional support of AAPI President Dr. Anupama Gotimukula and the Executive Committee Members, the relentless work of Members of the JAAPI Editorial Board, Editorial Advisors, and Reviewers as well as Ms. Vijaya Kodali, the Chief Operations Officer of AAPI.” “This is a historical milestone in the annals of AAPI. The foundation for this milestone was laid one year ago in February 2020 by our visionary leaders, Drs. Sudhakar Jonnalagadda and Suresh Reddy,” said Dr. Kishore, said. Describing the vision and the efforts that have given shape to the launching of JAAPI, Dr. Kishore said, “A Peer Review Journal needs group synergy and cultivation of the culture of peer-review process and publication. It is like agriculture – crop after crop. But the very fact that we are able to assemble a passionate and diligent team of editorial board members, and developed the required group synergy and culture bringing out the journal as planned, itself is a sign that AAPI has reached a level of academic maturity, capability and perfection.”
“This is a historical milestone in the annals of AAPI. The foundation for this milestone was laid one year ago in February 2020 by our visionary leaders, Drs. Sudhakar Jonnalagadda and Suresh Reddy,” said Dr. Kishore, said. Describing the vision and the efforts that have given shape to the launching of JAAPI, Dr. Kishore said, “A Peer Review Journal needs group synergy and cultivation of the culture of peer-review process and publication. It is like agriculture – crop after crop. But the very fact that we are able to assemble a passionate and diligent team of editorial board members, and developed the required group synergy and culture bringing out the journal as planned, itself is a sign that AAPI has reached a level of academic maturity, capability and perfection.” Dr. Santosh Kumar said that this brick-and-mortar University is being built on a 38 plus acre campus and will offer Certification, Associate, Bachelor, Masters and PHD degree courses in a formal setting. Dr. Santosh Kumar said that with this giant step, she is fulfilling her lifelong dream to globally promote the precious knowledge of Vedic Scriptures, Science of Upanishads and Hindu Philosophy to all. Dr. Santosh Kumar said that initial funding of this University will be from her late husband Pramod Kumar’s Trust fund and her family personally.
Dr. Santosh Kumar said that this brick-and-mortar University is being built on a 38 plus acre campus and will offer Certification, Associate, Bachelor, Masters and PHD degree courses in a formal setting. Dr. Santosh Kumar said that with this giant step, she is fulfilling her lifelong dream to globally promote the precious knowledge of Vedic Scriptures, Science of Upanishads and Hindu Philosophy to all. Dr. Santosh Kumar said that initial funding of this University will be from her late husband Pramod Kumar’s Trust fund and her family personally. However, even if the ban is ultimately blocked, it will have a lasting impact on Texas and provide a roadmap for other conservative states to enact similar abortion restrictions. Senate Bill 8, signed by Republican Gov. Greg Abbott in May, bars abortions once a doctor can detect fetal cardiac activity, which is often before many people know they are pregnant. The ban would prevent at least 85% of abortions sought in Texas, according to abortion rights advocates and providers. It is now the most restrictive abortion law in the nation; at least 12 other states have passed six-week abortion bans, but all have been blocked from going into effect. “Texas politicians will have effectively overturned Roe v. Wade,” Nancy Northup, president and CEO of the Center for Reproductive Rights, said shortly before the law went into effect, referring to the landmark 1973 decision that established the constitutionally protected right to abortion before a fetus is viable.
However, even if the ban is ultimately blocked, it will have a lasting impact on Texas and provide a roadmap for other conservative states to enact similar abortion restrictions. Senate Bill 8, signed by Republican Gov. Greg Abbott in May, bars abortions once a doctor can detect fetal cardiac activity, which is often before many people know they are pregnant. The ban would prevent at least 85% of abortions sought in Texas, according to abortion rights advocates and providers. It is now the most restrictive abortion law in the nation; at least 12 other states have passed six-week abortion bans, but all have been blocked from going into effect. “Texas politicians will have effectively overturned Roe v. Wade,” Nancy Northup, president and CEO of the Center for Reproductive Rights, said shortly before the law went into effect, referring to the landmark 1973 decision that established the constitutionally protected right to abortion before a fetus is viable. Does eating breakfast help you lose weight?
Does eating breakfast help you lose weight? People who tested positive for SARS-CoV-2 after one or two vaccine doses had significantly lower odds of severe disease or hospitalisation than unvaccinated people, according to a large-scale study investigating COVID-19 breakthrough infections published in The Lancet Infectious Diseases journal. Researchers also found that the odds of experiencing long COVID (illness lasting 28 days or more after a positive test) were cut in half for people who received two vaccines doses.
People who tested positive for SARS-CoV-2 after one or two vaccine doses had significantly lower odds of severe disease or hospitalisation than unvaccinated people, according to a large-scale study investigating COVID-19 breakthrough infections published in The Lancet Infectious Diseases journal. Researchers also found that the odds of experiencing long COVID (illness lasting 28 days or more after a positive test) were cut in half for people who received two vaccines doses.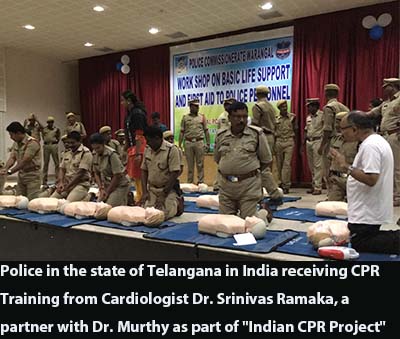 Affiliated with various US medical organizations and institutions, the soft-spoken Dr. Murthy is a Resuscitation Educator and Researcher, Advisor to Resuscitation Training Centers, Champion of Community Cardiopulmonary Resuscitation (CPR), and a Leader of US Organized Medicine. His Mission has been “Saving Lives” in Sudden Cardiac Arrests and common heart issues.
Affiliated with various US medical organizations and institutions, the soft-spoken Dr. Murthy is a Resuscitation Educator and Researcher, Advisor to Resuscitation Training Centers, Champion of Community Cardiopulmonary Resuscitation (CPR), and a Leader of US Organized Medicine. His Mission has been “Saving Lives” in Sudden Cardiac Arrests and common heart issues.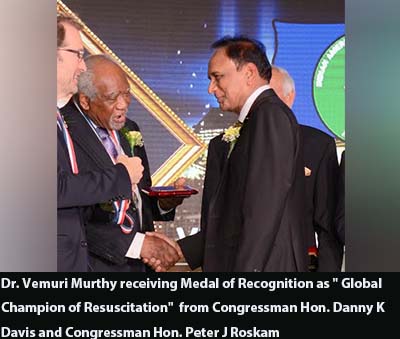 The Founder of Chicago Medical Society’s Community CPR Project Saving More Illinois Lives through Education (SMILE,) Dr. Murthy, takes upon himself the life-long mission of saving lives through effective preventive measures. He says, “Almost one in three among South Asians may die from heart disease before 65 years of age.”
The Founder of Chicago Medical Society’s Community CPR Project Saving More Illinois Lives through Education (SMILE,) Dr. Murthy, takes upon himself the life-long mission of saving lives through effective preventive measures. He says, “Almost one in three among South Asians may die from heart disease before 65 years of age.” Dr. Murthy served the American Heart Association in different capacities. Such as National and International Faculty, Member of the International Committee, and Advisor to AHA International Training Centers, Also as AHA Liaison to Medical Organizations in the USA too. He co-chaired programs at the AHA Scientific Sessions and delivered Resuscitation-based lectures at prestigious US medical institutions.
Dr. Murthy served the American Heart Association in different capacities. Such as National and International Faculty, Member of the International Committee, and Advisor to AHA International Training Centers, Also as AHA Liaison to Medical Organizations in the USA too. He co-chaired programs at the AHA Scientific Sessions and delivered Resuscitation-based lectures at prestigious US medical institutions. China
China “In previous studies, viral load has been used as an indirect measure of transmission,” says Dr.
“In previous studies, viral load has been used as an indirect measure of transmission,” says Dr.  U.S. Surgeon General Dr. Vivek Murthy has defended the Biden administration’s plans to
U.S. Surgeon General Dr. Vivek Murthy has defended the Biden administration’s plans to  In his presidential address, while expressing gratitude to the members of AKMG “for giving me the opportunity this year to be the President of our wondrous organization”. Dr. Subrahmanya Bhat said, “I worked very hard to make sure that this year’s AKMG was the best it could be. Likewise, our executive team has worked very hard to make sure the convention would be successful and profitable. Despite the challenges posed by the pandemic.”
In his presidential address, while expressing gratitude to the members of AKMG “for giving me the opportunity this year to be the President of our wondrous organization”. Dr. Subrahmanya Bhat said, “I worked very hard to make sure that this year’s AKMG was the best it could be. Likewise, our executive team has worked very hard to make sure the convention would be successful and profitable. Despite the challenges posed by the pandemic.” While inaugurating the convention with the traditional lighting of the lamp, in her keynote address, Dr. Swathi Kulkarni, Consul General of India in Atlanta, described the Indian American Physician community as a “Testament to the greatest growth story”. While emphasizing the role of physicians during the pandemic, Dr. Kulkarni praised their contributions and achievements. Dr. Kulkarni shared with the audience about the many programs and plans offered by the Government of India. Those are to alleviate the sufferings of the people of India during the pandemic. In addition, Dr. Kulkarni stressed the importance of the Indo-US Strategic Alliance, especially in the health sector. While pointing out India’s contributions to providing the world with quality drugs for lower prices.
While inaugurating the convention with the traditional lighting of the lamp, in her keynote address, Dr. Swathi Kulkarni, Consul General of India in Atlanta, described the Indian American Physician community as a “Testament to the greatest growth story”. While emphasizing the role of physicians during the pandemic, Dr. Kulkarni praised their contributions and achievements. Dr. Kulkarni shared with the audience about the many programs and plans offered by the Government of India. Those are to alleviate the sufferings of the people of India during the pandemic. In addition, Dr. Kulkarni stressed the importance of the Indo-US Strategic Alliance, especially in the health sector. While pointing out India’s contributions to providing the world with quality drugs for lower prices. Being away from home, the participants were led to celebrate
Being away from home, the participants were led to celebrate  Dr. Sunil Kumar, Chair, AKMG Humanitarian Services, thanked AKMG members as they “stepped up to the plate when our motherland was crying for help. I have always been proud of AKMG’s commitment to charity and even more today with your actions. As you know, when the COVID second wave started threatening India, we came together and helped our people prevent a catastrophe. As a result, we were able to reach an agreement with the international charity organization GLOBAL MEDIC to match our donations with $100,000 worth of PPE equipment.”
Dr. Sunil Kumar, Chair, AKMG Humanitarian Services, thanked AKMG members as they “stepped up to the plate when our motherland was crying for help. I have always been proud of AKMG’s commitment to charity and even more today with your actions. As you know, when the COVID second wave started threatening India, we came together and helped our people prevent a catastrophe. As a result, we were able to reach an agreement with the international charity organization GLOBAL MEDIC to match our donations with $100,000 worth of PPE equipment.” A resident of Shrewsbury, MA, Dr. Abraham is a Professor of Medicine at the University of Massachusetts Medical School, Chief of Medicine and Emeritus President of the Medical staff at Saint Vincent Hospital, and Adjunct Professor of Medicine at Massachusetts College of Pharmacy and Health Services.
A resident of Shrewsbury, MA, Dr. Abraham is a Professor of Medicine at the University of Massachusetts Medical School, Chief of Medicine and Emeritus President of the Medical staff at Saint Vincent Hospital, and Adjunct Professor of Medicine at Massachusetts College of Pharmacy and Health Services. “The election of Dr. George Abraham to be the President of ACP is a testament to the leadership qualities, vision and passion Indian American physicians have come to be asscociuated with in the United States,” added Dr. Naresh Parikh. “I am proud of our community of Indian physicians for all the progress that we have made over the years,” said Dr. Kusum Punjabi, Chair of AAPI BOT. “In patient care, administration, leadership, or academics, we have excelled in the respective fields, holding important positions across the United States and the world.”
“The election of Dr. George Abraham to be the President of ACP is a testament to the leadership qualities, vision and passion Indian American physicians have come to be asscociuated with in the United States,” added Dr. Naresh Parikh. “I am proud of our community of Indian physicians for all the progress that we have made over the years,” said Dr. Kusum Punjabi, Chair of AAPI BOT. “In patient care, administration, leadership, or academics, we have excelled in the respective fields, holding important positions across the United States and the world.” The spectrum of these ailments is wide and deep, with many tricky “masqueraders” in the mix creating confusion, potential misdiagnoses, and faulty or poor treatment, and causing immeasurable suffering for millions of people. Dr. Ruchi Gupta, a world-renowned researcher and physician on the front lines of this silent epidemic, in her first book, shares revolutionary research from her lab to address the entire spectrum of food-related health conditions.
The spectrum of these ailments is wide and deep, with many tricky “masqueraders” in the mix creating confusion, potential misdiagnoses, and faulty or poor treatment, and causing immeasurable suffering for millions of people. Dr. Ruchi Gupta, a world-renowned researcher and physician on the front lines of this silent epidemic, in her first book, shares revolutionary research from her lab to address the entire spectrum of food-related health conditions. The book has won excellent reviews from well-known authors. David Perlmutter, MD, Fellow, American College of Nutrition, author, #1 New York Times bestseller Grain Brain and Brain Wash, wrote of the book: “Food Without Fear explores how our individual uniqueness plays into how we respond to the information that our food choices purvey. And the dichotomy between “good” and “bad” foods is explored through the lenses of both leading edge science as well as our food-related responses. Both these data sets empower the reader with tools to optimize food choices and pave the way for a healthier life.”
The book has won excellent reviews from well-known authors. David Perlmutter, MD, Fellow, American College of Nutrition, author, #1 New York Times bestseller Grain Brain and Brain Wash, wrote of the book: “Food Without Fear explores how our individual uniqueness plays into how we respond to the information that our food choices purvey. And the dichotomy between “good” and “bad” foods is explored through the lenses of both leading edge science as well as our food-related responses. Both these data sets empower the reader with tools to optimize food choices and pave the way for a healthier life.” In New York City, the ‘Key to NYC Pass’ mandate began on Monday, which requires diners to show proof of at least one vaccination dose in order to dine indoors at restaurants, reports Xinhua news agency.
In New York City, the ‘Key to NYC Pass’ mandate began on Monday, which requires diners to show proof of at least one vaccination dose in order to dine indoors at restaurants, reports Xinhua news agency. “Thanks to God and to the work of many, we now have vaccines to protect us from COVID-19. They grant us the hope of ending the pandemic, but only if they are available to all and if we work together,” the pope wrote in the message addressed to all people on the vaccination campaign against COVID-19.
“Thanks to God and to the work of many, we now have vaccines to protect us from COVID-19. They grant us the hope of ending the pandemic, but only if they are available to all and if we work together,” the pope wrote in the message addressed to all people on the vaccination campaign against COVID-19. “FOOD WITHOUT FEAR: Identify, Prevent, and Treat Food Allergies, Intolerances, and Sensitivities,” a newly released book by Dr. Ruchi Gupta, an young and talented Indian American, illuminates what she has coined the food reaction spectrum—a revolutionary way to look at food-related conditions—and offers a new approach to managing adverse responses to food with a practical plan to end the misery and enjoy eating with ease.
“FOOD WITHOUT FEAR: Identify, Prevent, and Treat Food Allergies, Intolerances, and Sensitivities,” a newly released book by Dr. Ruchi Gupta, an young and talented Indian American, illuminates what she has coined the food reaction spectrum—a revolutionary way to look at food-related conditions—and offers a new approach to managing adverse responses to food with a practical plan to end the misery and enjoy eating with ease. Dr. Gupta is world-renowned for her groundbreaking research in the areas of food allergy and asthma epidemiology, most notably for her research on the prevalence of pediatric and adult food allergy in the United States. She has also significantly contributed to academic research in the areas of food allergy prevention, socioeconomic disparities in care, and the daily management of these conditions. Dr. Gupta is the author of The Food Allergy Experience, has written and co-authored over 150 peer-reviewed research manuscripts, and has had her work featured on major TV networks and in print media.
Dr. Gupta is world-renowned for her groundbreaking research in the areas of food allergy and asthma epidemiology, most notably for her research on the prevalence of pediatric and adult food allergy in the United States. She has also significantly contributed to academic research in the areas of food allergy prevention, socioeconomic disparities in care, and the daily management of these conditions. Dr. Gupta is the author of The Food Allergy Experience, has written and co-authored over 150 peer-reviewed research manuscripts, and has had her work featured on major TV networks and in print media. “I’ll be surprised if we don’t see 200,000 cases a day over the next two weeks, and it’s heartbreaking considering we never thought we would be back in this space,” said Dr Francis. Collins on Fox News Sunday, August 15th.
“I’ll be surprised if we don’t see 200,000 cases a day over the next two weeks, and it’s heartbreaking considering we never thought we would be back in this space,” said Dr Francis. Collins on Fox News Sunday, August 15th. “On the occasion of the 75thIndependence Day of India, we the physicians of Indian origin serving every 7th patient in the United States, is excited to launch this unique and noble initiative in collaboration with Bitcare, ‘AAPI Blood Donation and Stem Cell Drive” in 75 cities across the United States,” Dr. Gotimukula added.
“On the occasion of the 75thIndependence Day of India, we the physicians of Indian origin serving every 7th patient in the United States, is excited to launch this unique and noble initiative in collaboration with Bitcare, ‘AAPI Blood Donation and Stem Cell Drive” in 75 cities across the United States,” Dr. Gotimukula added. Blood saves lives. Blood is needed every two seconds. Nearly 21 million blood components are transfused in the U.S. every year. While not everyone is able to donate blood, Dr. Gotimukula pointed out that only 37 percent of the country’s population is able to donate blood. On why she and the AAPI leadership chose this as a priority\, Dr. Gotiumuka said, “The 3rd Covid Wave is causing increased ICU admissions again. There is a dire need for blood. Your friends or family may need your blood someday. And this noble cause helps save many lives.”
Blood saves lives. Blood is needed every two seconds. Nearly 21 million blood components are transfused in the U.S. every year. While not everyone is able to donate blood, Dr. Gotimukula pointed out that only 37 percent of the country’s population is able to donate blood. On why she and the AAPI leadership chose this as a priority\, Dr. Gotiumuka said, “The 3rd Covid Wave is causing increased ICU admissions again. There is a dire need for blood. Your friends or family may need your blood someday. And this noble cause helps save many lives.” Describing the benefits of Blood Donation, Dr. Gotiumukula said, a single donation can save three lives. Each blood component of whole blood transfusion can help up to three different people. Pointing to the fact that Blood cannot be manufactured, The President of AAPI said, “Despite medical and technological advances, blood cannot be made, so donations are the only way we can give blood to those who need it.”
Describing the benefits of Blood Donation, Dr. Gotiumukula said, a single donation can save three lives. Each blood component of whole blood transfusion can help up to three different people. Pointing to the fact that Blood cannot be manufactured, The President of AAPI said, “Despite medical and technological advances, blood cannot be made, so donations are the only way we can give blood to those who need it.” Though these prominent cyber incidents have triggered several cybersecurity initiatives, policymakers have paid relatively little attention to the considerable potential cyber risks in the healthcare sector. The
Though these prominent cyber incidents have triggered several cybersecurity initiatives, policymakers have paid relatively little attention to the considerable potential cyber risks in the healthcare sector. The  “We recognize that for some, the FDA approval of COVID-19 vaccines may bring additional confidence and encourage them to get vaccinated,” Abigail Capobianco, a spokeswoman at the FDA, said in a statement on Aug. 4. “Acknowledging the urgency related to the current state of the pandemic, we have taken an all-hands-on-deck approach, including identifying additional resources such as personnel and technological resources from across the agency and opportunities to reprioritize other activities, in order to complete our review to help combat this pandemic surge.”
“We recognize that for some, the FDA approval of COVID-19 vaccines may bring additional confidence and encourage them to get vaccinated,” Abigail Capobianco, a spokeswoman at the FDA, said in a statement on Aug. 4. “Acknowledging the urgency related to the current state of the pandemic, we have taken an all-hands-on-deck approach, including identifying additional resources such as personnel and technological resources from across the agency and opportunities to reprioritize other activities, in order to complete our review to help combat this pandemic surge.” The agency said the halt should last at least two months, to give the world a chance to meet the director-general’s goal of vaccinating 10% of the population of every country by the end of September.
The agency said the halt should last at least two months, to give the world a chance to meet the director-general’s goal of vaccinating 10% of the population of every country by the end of September. Shicowich lost his toe because of complications of Type 2 diabetes as he struggled to keep his blood sugar under control. He was overweight and on diabetes medications, but his diet of fast food and convenient, frozen processed meals had pushed his disease to life-threatening levels.
Shicowich lost his toe because of complications of Type 2 diabetes as he struggled to keep his blood sugar under control. He was overweight and on diabetes medications, but his diet of fast food and convenient, frozen processed meals had pushed his disease to life-threatening levels.