
We strive to help you make smarter purchasing decisions. While we adhere to strict editorial integrity, this post may contain references to products from our partners. Here’s an explanation for how we make money.
The COVID-19 pandemic has changed the world and our lives in so many ways, and for so many of us, this time that was largely spent at home staying safe also meant indulging in comfort foods. As a result of this, many Americans have gained weight over the last year. One study of 3,000 Americans done by the American Psychological Association found that 61 percent of respondents had an unwanted weight change during COVID.
 The thing is, yes, our bodies may have changed in ways we didn’t want them to, but the most important thing to remember is that our bodies also got us through a global pandemic, and that’s something to be grateful for. But with the new working-from-home lifestyle, elevated stress levels, and gym closures that we all faced during the pandemic, it means that some have put on a few pounds. Other than the extra weight being an annoyance, it can also lead to other lifestyle hiccups, like sleep, for instance. Weight fluctuations, believe it or not, can affect your sleep hygiene, so it’s important to understand how weight, stress, and sleep go hand in hand (in hand), so you can make sure you’re still getting enough sleep at night, even with a change in lifestyle and health.
The thing is, yes, our bodies may have changed in ways we didn’t want them to, but the most important thing to remember is that our bodies also got us through a global pandemic, and that’s something to be grateful for. But with the new working-from-home lifestyle, elevated stress levels, and gym closures that we all faced during the pandemic, it means that some have put on a few pounds. Other than the extra weight being an annoyance, it can also lead to other lifestyle hiccups, like sleep, for instance. Weight fluctuations, believe it or not, can affect your sleep hygiene, so it’s important to understand how weight, stress, and sleep go hand in hand (in hand), so you can make sure you’re still getting enough sleep at night, even with a change in lifestyle and health.
If you’ve found that you’ve recently experienced a change in weight and your sleep has been affected as a result of it (or if you just want some assistance in finding better sleep), we’ve put together a guide on understanding your new body and how it can affect the rest of your lifestyle.
The Pandemic’s Negative Effects on Weight Gain and Healthy Sleep
The COVID-19 pandemic, to put it simply, has been awful. Not only has it had a huge, negative impact on the world as a whole, but it’s been incredibly stressful (and dangerous) for people everywhere. This stress over the past year has had a direct result on your sleep, whether you’ve realized it or not. Dubbed “coronasomnia,” this COVID-related sleeplessness has been difficult to battle, but stress is only one factor here.
Stress is actually related to why so many people have gained weight over the last year, along with lack of activity. While we were all playing it safe by staying home to avoid getting sick, many of us were also not moving very much. Suddenly many people are working from home and falling into a totally different lifestyle from what they were used to.
The APA survey found that the average amount of weight gain over the last year was 29 pounds, but answers varied greatly. The survey also asked about how the pandemic affected mental health, and many said they felt a negative impact. When your mental health suffers, so much can go right along with it, including your physical health. During this time, when there was so much uncertainty, many found comfort in things like food or curling up on the couch with Netflix. While those might provide immediate comfort, it also leads to weight gain, which can have further negative effects on your body.
Other pandemic habits that could have negatively affected your weight include:
Your work-from-home lifestyle: Working from home means you aren’t getting any movement you might have gotten from a commute. Even if you drive to and from work, you aren’t getting up in the morning and doing a morning routine, walking to your car, walking into work, and reversing it at the end of the day. A WFH lifestyle has been appealing for many because you got time back in your day, but it also meant less activity.
Being stuck indoors: For many people, their activity was an outdoor thing. For much of the last year, we’ve been staying indoors, which cut out outdoor activities that increased exercise. As the virus started to wane, people were able to get outside more and more, but that was only after several months of staying inside. The benefits of being outdoors are not only great for physical health but mental health, as well.
Gym closures: Gyms and fitness centers were closed for a long time, and if that was your only way of working out, you might have lost out on your exercise time. Not everyone has the space or means to work out at home, so maybe you took a break from calorie-burning. That’s okay!
Many things could have gone into your weight gain over the past year, and, again, the most important thing to remember right now is that you’re here, you’ve made it through this pandemic, and you want to live a healthy lifestyle, and that means making sure you’re paying attention to your sleep hygiene, even with a little bit of extra weight on you. Don’t worry, we’ve got you covered on everything you need to know.
How Weight Gain Can Impact Your Ability to Sleep
An unfortunate side effect of gaining weight is disrupted sleep. It can happen for a variety of reasons, but many of these factors can be tied back to a change in your weight. Just like other factors in your life can affect how you sleep at night, a change in your body in any form definitely can. Here’s a look at how weight affects your sleep hygiene.
Sleep apnea
Sleep apnea is what occurs when you momentarily stop breathing while you’re asleep. Studies have shown that sleep apnea can occur for a number of reasons, one of which is an elevated weight. If you’re an older man, you’re also at a higher risk for sleep apnea, and weight gain can only make you more at risk for this sleep disorder. Sleep apnea can be very dangerous if left untreated, so if you have any suspicion that you’re dealing with this (snoring, insomnia, and morning headaches are all symptoms), check with your doctor for treatment.
Discomfort while sleeping
If you’ve put on a significant amount of weight, you might feel uncomfortable while sleeping. This can be from added strain on your body from the extra weight. Your joints probably aren’t used to some extra weight on them, and that can make you uncomfortable while you’re sleeping. If you’re not comfortable, you won’t sleep well. One way to combat this is with a more comfortable sleeping environment, like with a better mattress and supportive pillows.
Added stress
This is a vicious cycle. The pandemic has certainly added stress to your life, which may have contributed to your weight gain, and the stress and weight gain can make it more difficult to sleep at night. Without a good night of sleep, you’re more likely to make poor food choices during the day and be more stressed because you’re tired, continuing the cycle. Stress wreaks so much havoc on your sleep patterns, so it’s important to do whatever you can to cut back on stress in the way that works best for you.
A way to target all of these sleep issues is, of course, to work toward a healthy weight goal, but we know that’s easier said than done and not necessarily a priority for everyone. Studies have shown that a decrease in belly fat is linked to better sleep, but it’s virtually impossible to target belly fat when working out or eating healthy. While you can tone certain muscles with weight lifting, you can’t reduce fat on your body. So if you want to reduce belly fat, you simply have to eat healthily and exercise — the fat will come off everywhere, including your belly.
Your weight also factors into your Body Mass Index (BMI), and while this metric is often viewed as wildly outdated and irrelevant, studies have analyzed how it equates to sleep patterns. One study showed that people who had a lower BMI slept longer hours than those with a higher BMI. A healthy BMI range is considered to be about 18.5 to 25. While it can be a goal to aim for what is considered a healthy BMI on the scale, your better bet is to either consult your own healthcare provider on what a healthy weight is for you or simply work toward a level of health that is attainable and maintainable.
Tips for Achieving Better Sleep
No matter what your concern, there are always ways to improve your sleeping habits. It may take some trial and error to figure out what tips will work for you, but good sleep is worth the effort. Here are a few things you can try.
Set a consistent bedtime
This is one of the best things you can do to improve sleep. Create a routine for yourself that starts with bedtime preparation. Maybe it includes a warm bath, and maybe it includes reading a few pages, maybe it includes listening to some music. All of these can help you wind down, but whatever you have to do, make sure you’re climbing into bed around the same time every night. Ideally, you want to get in bed in enough time for a complete night of sleep (depending on age, this could vary from seven to 10 hours for people over the age of 13).
Consider what time you need to wake up in the morning and work your way back from there to set your bedtime, and stick to that. This routine will help get your body in the mode for bedtime on a regular basis.
Avoid snacking before bed
While some foods can help you sleep, eating the wrong foods before bed is more of a bad idea than a good one. Some foods can lead to indigestion or prolonged wakefulness. If you’re very hungry and it’s nearing bedtime, reach for foods with natural melatonin or things that will sit well in your stomach as you’re falling asleep.
Create a den of comfort
If your bed isn’t comfortable, you won’t sleep well, plain and simple. Make sure you have a mattress that’s appropriate for your sleeping style, as well as any bells and whistles you might need. These could be mattress toppers for more comfort, pillows that better support your neck, or even an adjustable bed base to elevate you. Though these changes in your bed can come with a price tag, there are plenty of affordable options for mattresses, pillows, and accessories. For the best sleep, it’s important to create a comfortable and supportive sleeping environment.
If your weight has changed, it might make your mattress feel completely different than it used to. Different mattress constructions will hold your weight differently, and if you’re heavier, you’ll sink into the mattress more. On some mattresses, that means you have less support than you once did.
It’s important to consider your weight when shopping for a mattress and understanding how different mattresses feel for different body types. Someone who is incredibly petite will have a different sleeping experience than someone who is of average weight. If you’re on the heavier side, you want to find a mattress that will support you for a long period of time and not break down or start to sag. There are mattresses on the market designed for people of larger stature so you can be sure you’re getting a supportive night of quality sleep. In general, these mattresses are hybrids made with coils or innersprings. Foam mattresses don’t provide proper support for larger people, which is why looking for a mattress with a spring or coil core is a better option.
If you’re struggling with sleep and think changing your mattress could help, it’s worth looking into a properly supportive mattress for your sleeping style or even your weight.
Consider the season
The time of year can absolutely affect how well you sleep. If it’s cold season, that can make it harder to breathe or sleep comfortably during the night. If it’s allergy season, you might also have a hard time breathing at night. While it can be tricky to really do much about something like a cold or allergies, it’s worth keeping them in mind if insomnia is knocking at your door. Do what you can to remedy any of these seasonal annoyances, like by using a humidifier or dehumidifier (depending on your concern) while you sleep or adding some melatonin into your bedtime routine to make sleeping easier.
Exercise
Yes, exercise will definitely help you sleep. You can look at it in a few different ways. One, exercise can be a great stress relief, and less stress usually means better sleep. Exercise also, quite simply, makes you tired. (Though you don’t want to exercise right before bed because your body doesn’t have enough time to cool down and head into the proper circadian rhythm.) Exercising during the day raises your heart rate and encourages the release of melatonin into the body, keeping your circadian rhythm running smoothly — which all contribute to a restful night of sleep.
And of course, we know exercise is a great way to burn off some calories, which can be helpful if you’re carrying a little extra weight that you don’t want. It doesn’t take much to get your heart rate up and break a sweat. Even a simple walk each day is beneficial for all these factors that contribute to better sleep.
Cut the screens
Ditch your phones, TVs, and tablets before bedtime. Though it’s not a big deal to use your gadgets earlier in the evening, once you get in bed, you should put them away or turn them off. The harsh light makes it harder to sleep, and we all know how addicting it can be to continuously scroll through social media. Put them away when you get in bed and reset your mind for sleep instead.
Closing
The most important thing you can remember from all of this is that your body got you through a pandemic. So maybe it looks a little different today than it did a year ago. Bodies change all the time, and you have to give yourself a little bit of grace. Though weight fluctuations can affect your lifestyle, including your sleep hygiene, it’s a manageable concern that you can definitely get through. You’re still here, and you’re open to finding ways to make changes. That’s what matters.
 “The generosity of the members of AAPI and Indian community has been unprecedented,” says Dr. Anupama Gotimukula, President of AAPI. “I want to thank the AAPI fraternity, for not only contributing $5 Million towards Covid Relief Funds, but has spent hundreds of hours in coordinating and disbursing the vital medical supplies to the most needed hospitals across India.”
“The generosity of the members of AAPI and Indian community has been unprecedented,” says Dr. Anupama Gotimukula, President of AAPI. “I want to thank the AAPI fraternity, for not only contributing $5 Million towards Covid Relief Funds, but has spent hundreds of hours in coordinating and disbursing the vital medical supplies to the most needed hospitals across India.” Ram N Kumar, the founder of NirogStreet, has told the media that he was fortunate to find a clutch of investors from the US, who could not just invest but guide. “For me, if you get a person like Gokul to help you while building a company, it is a once in a lifetime opportunity,” Kumar said.
Ram N Kumar, the founder of NirogStreet, has told the media that he was fortunate to find a clutch of investors from the US, who could not just invest but guide. “For me, if you get a person like Gokul to help you while building a company, it is a once in a lifetime opportunity,” Kumar said. “Women’s diets were lacking in diverse foods even before the pandemic, but COVID-19 has further exacerbated the situation,” said Soumya Gupta, a research economist at TCI who coauthored the study along with
“Women’s diets were lacking in diverse foods even before the pandemic, but COVID-19 has further exacerbated the situation,” said Soumya Gupta, a research economist at TCI who coauthored the study along with  Dr. Juthani is an infectious diseases physician at Yale School of Medicine in New Haven, where she specializes in the diagnosis, management, and prevention of infections in older adults. Her most recent area of interest is at the interface of infectious diseases and palliative care, including the role of antibiotics at the end of life, the press release from the Governor noted.
Dr. Juthani is an infectious diseases physician at Yale School of Medicine in New Haven, where she specializes in the diagnosis, management, and prevention of infections in older adults. Her most recent area of interest is at the interface of infectious diseases and palliative care, including the role of antibiotics at the end of life, the press release from the Governor noted.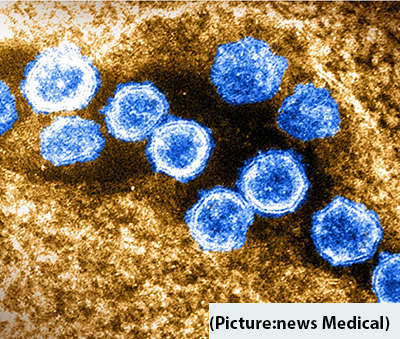 When a person is infected with COVID-19, antibodies are typically produced to fight against the invading disease. These antibodies are unique to each individual, meaning that some antibodies are better than others at combating the virus. Thus, pharmaceutical companies study thousands of these antibodies to take advantage of the most effective ones with the highest barrier to resistance.
When a person is infected with COVID-19, antibodies are typically produced to fight against the invading disease. These antibodies are unique to each individual, meaning that some antibodies are better than others at combating the virus. Thus, pharmaceutical companies study thousands of these antibodies to take advantage of the most effective ones with the highest barrier to resistance. This herb also contains cooling components thus making it really helpful for summers. It detoxifies the body and maintains one’s body temperature pace. Adding to the benefits Basil contains antioxidant-rich volatile essential oils, which are considered hydrophobic, meaning they don’t dissolve in water and are light and small enough to travel through the air and the pores within our skin. Basil’s volatile essential oil is something that gives the herb its distinct smell and taste, but basil contains some great healing properties.
This herb also contains cooling components thus making it really helpful for summers. It detoxifies the body and maintains one’s body temperature pace. Adding to the benefits Basil contains antioxidant-rich volatile essential oils, which are considered hydrophobic, meaning they don’t dissolve in water and are light and small enough to travel through the air and the pores within our skin. Basil’s volatile essential oil is something that gives the herb its distinct smell and taste, but basil contains some great healing properties. Ashwagandha (Withania Somnifera), commonly known as ‘Indian winter cherry’, is a traditional Indian herb that boosts energy, reduces stress, and makes the immune system stronger.
Ashwagandha (Withania Somnifera), commonly known as ‘Indian winter cherry’, is a traditional Indian herb that boosts energy, reduces stress, and makes the immune system stronger. Dr. Kusum Punjabi the Chair of Board of Trustees of AAPI, who is the youngest to date to be holding this position in AAPI’s 40 years long history and serving patients in the Emergency Department, said “As the pandemic has exhausted all the resources, especially the lifesaving and much needed Blood across the nation and the world, AAPI is in the forefront, once again, spreading the message for the need to donate blood and save lives.”
Dr. Kusum Punjabi the Chair of Board of Trustees of AAPI, who is the youngest to date to be holding this position in AAPI’s 40 years long history and serving patients in the Emergency Department, said “As the pandemic has exhausted all the resources, especially the lifesaving and much needed Blood across the nation and the world, AAPI is in the forefront, once again, spreading the message for the need to donate blood and save lives.” Dr. Krishan Kumar, a pediatric emergency medicine physician in East Meadow, New York and is affiliated with multiple hospitals in the area, quoting studies done on the need and usefulness of Blood said, “Blood donation helps save lives. In fact, every two seconds of every day, someone needs blood. Since blood cannot be manufactured outside the body and has a limited shelf life, the supply must constantly be replenished by generous blood donors.” The growing influence of physicians of Indian heritage is evident, as increasingly physicians of Indian origin hold critical positions in the healthcare, academic, research and administrative positions across the nation. We the physicians of Indian origin are proud of our great achievements and contributions to our motherland, India, our adopted land, the US and in a very significant way to the transformation of the Indo-US relations.
Dr. Krishan Kumar, a pediatric emergency medicine physician in East Meadow, New York and is affiliated with multiple hospitals in the area, quoting studies done on the need and usefulness of Blood said, “Blood donation helps save lives. In fact, every two seconds of every day, someone needs blood. Since blood cannot be manufactured outside the body and has a limited shelf life, the supply must constantly be replenished by generous blood donors.” The growing influence of physicians of Indian heritage is evident, as increasingly physicians of Indian origin hold critical positions in the healthcare, academic, research and administrative positions across the nation. We the physicians of Indian origin are proud of our great achievements and contributions to our motherland, India, our adopted land, the US and in a very significant way to the transformation of the Indo-US relations. “So it really is, as (Rochelle) Walensky (Director of the Centers for Disease Control and Prevention) has said many times and I have said, it is really a pandemic among the unvaccinated, so this is an issue predominantly among the unvaccinated, which is the reason why we’re out there, practically pleading with the unvaccinated people to go out and get vaccinated,” said the chief medical adviser to President Joe Biden.
“So it really is, as (Rochelle) Walensky (Director of the Centers for Disease Control and Prevention) has said many times and I have said, it is really a pandemic among the unvaccinated, so this is an issue predominantly among the unvaccinated, which is the reason why we’re out there, practically pleading with the unvaccinated people to go out and get vaccinated,” said the chief medical adviser to President Joe Biden. And as of July 23, the daily average of people becoming fully vaccinated was the lowest it had been since the end of January, the report said. Meanwhile, the CDC is also weighing the option of revising its Covid-19 guidelines to recommend that even fully vaccinated people wear masks in public, Fauci said.
And as of July 23, the daily average of people becoming fully vaccinated was the lowest it had been since the end of January, the report said. Meanwhile, the CDC is also weighing the option of revising its Covid-19 guidelines to recommend that even fully vaccinated people wear masks in public, Fauci said.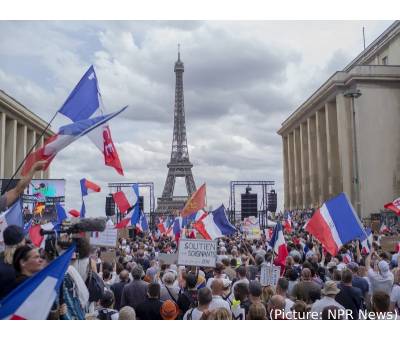 The bill was unveiled just six days ago. Lawmakers worked through the night and the weekend to reach a compromise version approved by the Senate on Sunday night and by the National Assembly after midnight. The rules can be applied through Nov. 15, depending on the virus situation. Macron appealed for national unity and mass vaccination to fight the resurgent virus, and lashed out at those fueling anti-vaccine sentiment and protests.
The bill was unveiled just six days ago. Lawmakers worked through the night and the weekend to reach a compromise version approved by the Senate on Sunday night and by the National Assembly after midnight. The rules can be applied through Nov. 15, depending on the virus situation. Macron appealed for national unity and mass vaccination to fight the resurgent virus, and lashed out at those fueling anti-vaccine sentiment and protests. The U.S. Centers for Disease Control and Prevention (CDC) placed a significant roadblock to such tailored management when it changed its
The U.S. Centers for Disease Control and Prevention (CDC) placed a significant roadblock to such tailored management when it changed its A full course of two of the most widely available coronavirus vaccines is about as effective against the more contagious delta variant as it was against a previously dominant version of the virus, according to
A full course of two of the most widely available coronavirus vaccines is about as effective against the more contagious delta variant as it was against a previously dominant version of the virus, according to  As a result, researchers expected another coronavirus epidemic or pandemic, though not necessarily one as bad as the COVID-19 outbreak. “This was the worst by far,” he said. Researchers anticipated the initial outbreak from China where the preceding epidemics occurred, but were surprised it came from Central China, not Southern China, as was the case with the 2002 SARS epidemic, he said.
As a result, researchers expected another coronavirus epidemic or pandemic, though not necessarily one as bad as the COVID-19 outbreak. “This was the worst by far,” he said. Researchers anticipated the initial outbreak from China where the preceding epidemics occurred, but were surprised it came from Central China, not Southern China, as was the case with the 2002 SARS epidemic, he said. In terms of the origin of patent applications in the pharma sector globally, India is among the top 10 countries, followed by Italy, Australia, Taiwan and Sweden. The applications originating from India are majorly filed in the US, European Parliament and APAC region. The top Indian filers who filed patents in India during the last five years (2015-2020) include the Council of Scientific and Industrial Research (CSIR), ITC Life Sciences, Lovely Professional University, Colgate Palmolive (India), Tata Consultancy Services (TCS) Limited, IIT Bombay, Cadila Healthcare, Lupin, Amity University, and Wockhardt Limited, the report said.
In terms of the origin of patent applications in the pharma sector globally, India is among the top 10 countries, followed by Italy, Australia, Taiwan and Sweden. The applications originating from India are majorly filed in the US, European Parliament and APAC region. The top Indian filers who filed patents in India during the last five years (2015-2020) include the Council of Scientific and Industrial Research (CSIR), ITC Life Sciences, Lovely Professional University, Colgate Palmolive (India), Tata Consultancy Services (TCS) Limited, IIT Bombay, Cadila Healthcare, Lupin, Amity University, and Wockhardt Limited, the report said. As the costs mounted, he borrowed from friends and relatives. Then, he turned to strangers, pleading online for help on Ketto, an Indian crowdfunding website. Overall, Sharma says he has paid over $50,000 in medical bills. The crowdfunding provided $28,000, but another $26,000 is borrowed money he needs to repay, a kind of debt he has never faced before. “He was struggling for his life and we were struggling to provide him an opportunity to survive,” he said, his voice thick with emotion. “I was a proud father — and now I have become a beggar.”
As the costs mounted, he borrowed from friends and relatives. Then, he turned to strangers, pleading online for help on Ketto, an Indian crowdfunding website. Overall, Sharma says he has paid over $50,000 in medical bills. The crowdfunding provided $28,000, but another $26,000 is borrowed money he needs to repay, a kind of debt he has never faced before. “He was struggling for his life and we were struggling to provide him an opportunity to survive,” he said, his voice thick with emotion. “I was a proud father — and now I have become a beggar.” The researchers conducted an online survey of nurses and other non-physician health care workers (HCWs), and received responses from 2,459 participants who provided direct patient care. The survey focused on risk factors for decreased well-being: a key contributor to the epidemic of burnout among health care professionals. The survey also evaluated aspects of resilience. Defined as the ability to cope with and adapt positively to adversity, resilience is an important contributor to well-being. Data were collected in June and July 2020, providing a snapshot of well-being and resilience among HCWs a few months into the pandemic.
The researchers conducted an online survey of nurses and other non-physician health care workers (HCWs), and received responses from 2,459 participants who provided direct patient care. The survey focused on risk factors for decreased well-being: a key contributor to the epidemic of burnout among health care professionals. The survey also evaluated aspects of resilience. Defined as the ability to cope with and adapt positively to adversity, resilience is an important contributor to well-being. Data were collected in June and July 2020, providing a snapshot of well-being and resilience among HCWs a few months into the pandemic. Rukmini S, a leading data journalist, has written that the numbers she’s gathered suggest a death toll closer to 2.5 million. A report from the Washington-based Center for Global Development think tank released Tuesday, July 20, 2021, studied data from three different sources, finding that excess deaths – a term public health experts use to describe mortality from all causes during a crisis that is above what would have been expected in ‘normal’ conditions – likely ranged between 3.4 million to 4.9 million.
Rukmini S, a leading data journalist, has written that the numbers she’s gathered suggest a death toll closer to 2.5 million. A report from the Washington-based Center for Global Development think tank released Tuesday, July 20, 2021, studied data from three different sources, finding that excess deaths – a term public health experts use to describe mortality from all causes during a crisis that is above what would have been expected in ‘normal’ conditions – likely ranged between 3.4 million to 4.9 million.
 Angela Rasmussen, a virologist and research scientist at the Vaccine and Infectious Disease Organization at the University of Saskatchewan has pointed to a compelling preprint study out of China recently that showed people who were exposed to the Delta variant got sick fast. The study has found that people infected with the Delta variant are shedding way more virus, which could explain why it’s so contagious. Rasmussen says the good news is that it still transmits in the same way as the original strain, so all of those mitigation tools like masking and handwashing and social distancing – all of those still work to block Delta. And the vaccines are still highly effective against this variant.
Angela Rasmussen, a virologist and research scientist at the Vaccine and Infectious Disease Organization at the University of Saskatchewan has pointed to a compelling preprint study out of China recently that showed people who were exposed to the Delta variant got sick fast. The study has found that people infected with the Delta variant are shedding way more virus, which could explain why it’s so contagious. Rasmussen says the good news is that it still transmits in the same way as the original strain, so all of those mitigation tools like masking and handwashing and social distancing – all of those still work to block Delta. And the vaccines are still highly effective against this variant. Born in Andhra Pradesh, India, Dr. Gangasani attended Kurnool Medical College (AP University of Health Sciences) from where he graduated in 1991. He was awarded State and National Merit Scholarships as well as Gold Medals and Merit Certificates in Pharmacology, Forensic Medicine, Social and Preventive Medicine and Internal Medicine for being a top- of- the- class student. He went on to win first place in Indian Academy of Pediatrics Quiz Competition. Later, in the U.S. he won Internal Medicine Quiz Competition as first year resident for internal residency program in 1994. He was also recognized Outstanding Resident in 1995. He won the first place in 1997 for presentation (Scientific paper Award) at Annual meeting of Michigan Association of Physicians from India.
Born in Andhra Pradesh, India, Dr. Gangasani attended Kurnool Medical College (AP University of Health Sciences) from where he graduated in 1991. He was awarded State and National Merit Scholarships as well as Gold Medals and Merit Certificates in Pharmacology, Forensic Medicine, Social and Preventive Medicine and Internal Medicine for being a top- of- the- class student. He went on to win first place in Indian Academy of Pediatrics Quiz Competition. Later, in the U.S. he won Internal Medicine Quiz Competition as first year resident for internal residency program in 1994. He was also recognized Outstanding Resident in 1995. He won the first place in 1997 for presentation (Scientific paper Award) at Annual meeting of Michigan Association of Physicians from India. Reasons for this recommendation include but are not limited to: a significant proportion of the student population is
Reasons for this recommendation include but are not limited to: a significant proportion of the student population is 
 Dr. Kusum Punjabi, a very young and energetic leader of AAPI, assumed office as the Chair of Board of Trustees of AAPI on July 4th. The youngest to date to be holding this position in AAPI’s 40 years long history and the first person to go to medical school in the USA, Dr. Punjabi completed her undergraduate degree from Rutgers University in Biology and Economics and graduated with high honors as a Henry Rutgers Scholar. She, then completed MD/MBA program from Rutgers Robert Wood Johnson Medical School and Rutgers Business School.
Dr. Kusum Punjabi, a very young and energetic leader of AAPI, assumed office as the Chair of Board of Trustees of AAPI on July 4th. The youngest to date to be holding this position in AAPI’s 40 years long history and the first person to go to medical school in the USA, Dr. Punjabi completed her undergraduate degree from Rutgers University in Biology and Economics and graduated with high honors as a Henry Rutgers Scholar. She, then completed MD/MBA program from Rutgers Robert Wood Johnson Medical School and Rutgers Business School. A recipient of several Community Service/Awards, Dr. Kathula wants to “Make AAPI a mainstream organization and work on issues affecting physicians including physician shortage, burnout, and credentialing, while leveraging the strength of 100,000 doctors at legislative level.” Another area, he wants to work is to “Encourage and engage next generation/young physicians in AAPI activities. While working closely with other physician organizations such as AMA.”
A recipient of several Community Service/Awards, Dr. Kathula wants to “Make AAPI a mainstream organization and work on issues affecting physicians including physician shortage, burnout, and credentialing, while leveraging the strength of 100,000 doctors at legislative level.” Another area, he wants to work is to “Encourage and engage next generation/young physicians in AAPI activities. While working closely with other physician organizations such as AMA.” A hospital in Springfield, Missouri, ran out of ventilators to treat hospitalized COVID patients over the weekend, local media reported. The city of 160,000’s two hospitals were treating 213 COVID-19 patients as of Monday, up from 168 on Friday and 31 on May 24, the Kansas City Star said. “The trajectory that we’re likely to see is two different flavours of the pandemic in the United States, one in which it’s more of a problem in places where there’s a high level of unvaccinated individuals,” Amesh Adalja of the Johns Hopkins Center for Health Security told AFP.
A hospital in Springfield, Missouri, ran out of ventilators to treat hospitalized COVID patients over the weekend, local media reported. The city of 160,000’s two hospitals were treating 213 COVID-19 patients as of Monday, up from 168 on Friday and 31 on May 24, the Kansas City Star said. “The trajectory that we’re likely to see is two different flavours of the pandemic in the United States, one in which it’s more of a problem in places where there’s a high level of unvaccinated individuals,” Amesh Adalja of the Johns Hopkins Center for Health Security told AFP. Apart from engaging in research activities, the centre publishes periodicals and books on Ayurveda, cultivates medicinal plants and organizes educational programmes. The founder, Dr P. S. Varier, started the Ayurveda Pathasala in 1917 which later became Vaidyaratnam P. S. Varier Ayurveda College. AVS also runs a Kathakali academy, named P. S. V. Natyasangham, where the classical dance form is taught and performed. P. S. V. Natyasangham is known for its strict adherence to the classical tenets of performance and meticulous training, and has produced talented artistes. A museum that preserves the personal belongings of Dr. Varier and documents the milestones in the history of Arya Vaidya Sala was established in 2002. It also chronicles the renaissance in the field of Ayurveda and its history.
Apart from engaging in research activities, the centre publishes periodicals and books on Ayurveda, cultivates medicinal plants and organizes educational programmes. The founder, Dr P. S. Varier, started the Ayurveda Pathasala in 1917 which later became Vaidyaratnam P. S. Varier Ayurveda College. AVS also runs a Kathakali academy, named P. S. V. Natyasangham, where the classical dance form is taught and performed. P. S. V. Natyasangham is known for its strict adherence to the classical tenets of performance and meticulous training, and has produced talented artistes. A museum that preserves the personal belongings of Dr. Varier and documents the milestones in the history of Arya Vaidya Sala was established in 2002. It also chronicles the renaissance in the field of Ayurveda and its history. Dr. Jonnalagadda, who had assumed office a year ago during a virtual convention, told the AAPI delegates, “Despite the Covid pandemic and the many challenges AAPI had to face, “I am proud of the many accomplishments under my leadership. I am grateful for the immense and life changing moments, probably the best of my life ever, that came with my association with and leading AAPI.” Describing how his own life has changed over the past years, he said, “Working with many physicians motivated me to be a better physician myself. I understood the higher meaning of being a physician, especially even more now during the COVID pandemic. AAPI has given me so much — networking, advocacy, and education — and I am honored to serve this noble organization. I sincerely appreciate the trust you placed in me as the President of AAPI, and I am deeply committed to continue to work for you.”
Dr. Jonnalagadda, who had assumed office a year ago during a virtual convention, told the AAPI delegates, “Despite the Covid pandemic and the many challenges AAPI had to face, “I am proud of the many accomplishments under my leadership. I am grateful for the immense and life changing moments, probably the best of my life ever, that came with my association with and leading AAPI.” Describing how his own life has changed over the past years, he said, “Working with many physicians motivated me to be a better physician myself. I understood the higher meaning of being a physician, especially even more now during the COVID pandemic. AAPI has given me so much — networking, advocacy, and education — and I am honored to serve this noble organization. I sincerely appreciate the trust you placed in me as the President of AAPI, and I am deeply committed to continue to work for you.” Dr. Jonnalagadda enumerated several programs under his leadership AAPI had undertaken in the past one year. “AAPI and the Charitable Foundation has several programs in India. Under my leadership with the pioneering efforts of Dr. SurenderPurohit, Chairman of AAPI CF, we have been able to strengthen the programs benefitting our motherland, India.” AAPI has been actively involved in community awareness programs like Obesity prevention, sharing medical knowledge at the weekly webinars on team building activities such as the Share a Blanket program, medical education programs such as CPR training, and educating the public and creating awareness on healthcare issues through ZeeTV and ITV Gold, NDTV, BBC, and CNN. Almost all the ethnic publications from coast to coast across the US and several leading publications in India have run timely stories on AAPI‘s several initiatives and programs.
Dr. Jonnalagadda enumerated several programs under his leadership AAPI had undertaken in the past one year. “AAPI and the Charitable Foundation has several programs in India. Under my leadership with the pioneering efforts of Dr. SurenderPurohit, Chairman of AAPI CF, we have been able to strengthen the programs benefitting our motherland, India.” AAPI has been actively involved in community awareness programs like Obesity prevention, sharing medical knowledge at the weekly webinars on team building activities such as the Share a Blanket program, medical education programs such as CPR training, and educating the public and creating awareness on healthcare issues through ZeeTV and ITV Gold, NDTV, BBC, and CNN. Almost all the ethnic publications from coast to coast across the US and several leading publications in India have run timely stories on AAPI‘s several initiatives and programs. AAPI has raised over $ 5 Million towards Covid relief funds for India and has purchased, shipped and coordinated with local authorities the supply and distribution of medical supplies to several parts of India. AAPI has shipped over a thousand Oxygen generators, masks, PPPs and essential supplies, and our pipeline will continue until the pandemic is overcome. As with anyone else, our doctors believe that they can best carry out our service to God through our service to our fellow humans.
AAPI has raised over $ 5 Million towards Covid relief funds for India and has purchased, shipped and coordinated with local authorities the supply and distribution of medical supplies to several parts of India. AAPI has shipped over a thousand Oxygen generators, masks, PPPs and essential supplies, and our pipeline will continue until the pandemic is overcome. As with anyone else, our doctors believe that they can best carry out our service to God through our service to our fellow humans. Delivering a spiritual discourse at the Convention, SadhviBhagawatiSaraswati, Author of “Hollywood to the Himalayas” led the AAPI delegates into an experience of peace and serenity. In her keynote address, Sadhviji inspired the participants to engage in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities professionals in the field of medicine. She emphasized the important and critical connection between mind and body by saying “As the Bhagavad Gita reminds us: the mind is the cause of all problems and the mind is, therefore, the solution.” She offered them a “Mantra” which she called, CURED, where C stands for Connections – Connect with your inner self; U stands for Understand that you are a tool in the hands of God; R stands for Reconnect with your inner self day in and day out; E stands for Equanimity – stay balanced in all you do; and, D stands for “Dhanyavad or Devotion” that is being grateful which will lead one to enjoy happiness kin life.
Delivering a spiritual discourse at the Convention, SadhviBhagawatiSaraswati, Author of “Hollywood to the Himalayas” led the AAPI delegates into an experience of peace and serenity. In her keynote address, Sadhviji inspired the participants to engage in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities professionals in the field of medicine. She emphasized the important and critical connection between mind and body by saying “As the Bhagavad Gita reminds us: the mind is the cause of all problems and the mind is, therefore, the solution.” She offered them a “Mantra” which she called, CURED, where C stands for Connections – Connect with your inner self; U stands for Understand that you are a tool in the hands of God; R stands for Reconnect with your inner self day in and day out; E stands for Equanimity – stay balanced in all you do; and, D stands for “Dhanyavad or Devotion” that is being grateful which will lead one to enjoy happiness kin life. Dr. Sudhir Parikh, CEO of Parikh Media introduced the keynote speaker, AnandibenMafatbhai Patel, an Indian politician serving as the 28th and current Governor of Uttar Pradesh. She also served as Governor of Madhya Pradesh. She has served as the former Chief Minister of Gujarat. She was the first female chief minister of the state, he said. In her virtual address, she congratulated AAPI for organizing the convention and thanked them for their selfless services to India, the US and the humanity. Dr. Bobby Mukkamala, Chair of BOT at American Medical Association shared with nostalgia his long association with AAPI, growing up as a child and now, be leading the largest Medical Association in the US. Aaishwariya A Gulani, Valedictorian from The International Bolles School and a 3rd year Medical Student having held leadership roles from academia as recognized by the United Nations to community service globally as the reigning Miss India USA participated in the Fashion Show.
Dr. Sudhir Parikh, CEO of Parikh Media introduced the keynote speaker, AnandibenMafatbhai Patel, an Indian politician serving as the 28th and current Governor of Uttar Pradesh. She also served as Governor of Madhya Pradesh. She has served as the former Chief Minister of Gujarat. She was the first female chief minister of the state, he said. In her virtual address, she congratulated AAPI for organizing the convention and thanked them for their selfless services to India, the US and the humanity. Dr. Bobby Mukkamala, Chair of BOT at American Medical Association shared with nostalgia his long association with AAPI, growing up as a child and now, be leading the largest Medical Association in the US. Aaishwariya A Gulani, Valedictorian from The International Bolles School and a 3rd year Medical Student having held leadership roles from academia as recognized by the United Nations to community service globally as the reigning Miss India USA participated in the Fashion Show. The concluding day of the convention had the usual pomp and show displayed in music and dance by the local organizing committee of the Convention headed by Dr. SreeniGangasani, who and his team were praised for their hardwork, dedication and creative ideas in putting together aan amazing convention in less than three months. “We are delighted to have been able to plan and organize the convention in record time,” said Dr. Gangasani. Calling it a historic convention, the Cardiologist from Atlanta said, “For the first time ever, we had to stop registration as we had reached the required number of participants for the convention, disappointing many who wanted to come and join the annual meet. Thank you for joining the AAPI community as we celebrate the victory of science over calamity while paying tribute to all the fallen healthcare workers including some from AAPI family. We also want to show the world that we can start socializing with precautions once you are vaccinated,” added Dr. Gangasani.
The concluding day of the convention had the usual pomp and show displayed in music and dance by the local organizing committee of the Convention headed by Dr. SreeniGangasani, who and his team were praised for their hardwork, dedication and creative ideas in putting together aan amazing convention in less than three months. “We are delighted to have been able to plan and organize the convention in record time,” said Dr. Gangasani. Calling it a historic convention, the Cardiologist from Atlanta said, “For the first time ever, we had to stop registration as we had reached the required number of participants for the convention, disappointing many who wanted to come and join the annual meet. Thank you for joining the AAPI community as we celebrate the victory of science over calamity while paying tribute to all the fallen healthcare workers including some from AAPI family. We also want to show the world that we can start socializing with precautions once you are vaccinated,” added Dr. Gangasani. AAPI recognized the current Executive Committee Members, BOT members and several others who have worked hard to make the vision and mission of AAPI come alive. Prominent among them are: Dr. Radhu Agrawal was bestowed with AAPI Lifetime Achievement Award; AAPI Most Distinguished Physician Award was given to Dr. DhanireddyRamasubbareddy; AAPI Most Distinguished Service Award was given to Dr. Suresh Gupta; AAPI Most Distinguished YPS Award went to Dr. Purvi Parikh; and, AAPI Most Distinguished Community Service was bestowed on Dr. Sujatha Reddy. Dr. Raghu Lolabhattu, Convention Vice Chair shared with the delegates about how in a matter of less than three months the Atlanta Chapter has put together a fabulous convention. He later on called on stage every member of the convention committee, while Dr. Lonnalagadda and Dr. Gangasani recognized them with a plaque. The past Presidents of were called on state on the 2nd night’s gala and were recognized for their leadership and continued guidance.
AAPI recognized the current Executive Committee Members, BOT members and several others who have worked hard to make the vision and mission of AAPI come alive. Prominent among them are: Dr. Radhu Agrawal was bestowed with AAPI Lifetime Achievement Award; AAPI Most Distinguished Physician Award was given to Dr. DhanireddyRamasubbareddy; AAPI Most Distinguished Service Award was given to Dr. Suresh Gupta; AAPI Most Distinguished YPS Award went to Dr. Purvi Parikh; and, AAPI Most Distinguished Community Service was bestowed on Dr. Sujatha Reddy. Dr. Raghu Lolabhattu, Convention Vice Chair shared with the delegates about how in a matter of less than three months the Atlanta Chapter has put together a fabulous convention. He later on called on stage every member of the convention committee, while Dr. Lonnalagadda and Dr. Gangasani recognized them with a plaque. The past Presidents of were called on state on the 2nd night’s gala and were recognized for their leadership and continued guidance. Some of these herbs and spices include turmeric, peppermint, ginger, and many more. Long before modern medicine, the ancient Greeks used a variety of spices and herbs for their healing properties.
Some of these herbs and spices include turmeric, peppermint, ginger, and many more. Long before modern medicine, the ancient Greeks used a variety of spices and herbs for their healing properties. 
 Dr. Smitha Lodha, widow of Dr. Ajay Lodha addressed the AAPI members, thanking them for their support as the late President of AAPI suffered Covid related complications and succumbed to the deadly virus. She praised AAPI and the medical fraternity for their courage and selfless service to bring health and well being to millions across the US and around the world.
Dr. Smitha Lodha, widow of Dr. Ajay Lodha addressed the AAPI members, thanking them for their support as the late President of AAPI suffered Covid related complications and succumbed to the deadly virus. She praised AAPI and the medical fraternity for their courage and selfless service to bring health and well being to millions across the US and around the world. After inaugurating the Convention with traditional prayers and blessings by Hindu Priests, Congressman Buddy Carter, representing the 1st District in Georgia, said, “If there is anything that the COVID-19 pandemic laid bare it is that our country is too dependent on foreign sources of critical pharmaceutical and medical supplies. I reintroduced bipartisan, bicameral legislation to retake control of America’s health care supply chain. For America’s national security, the legislation incentivizes the domestic manufacturing of drugs and other medical supplies to make the U.S. supply chain less dependent on foreign countries like China.” The only pharmacist in the US Congress, Rep. Carter referred to how the middlemen hike up the prize of drugs by upto 47% in the US, and urged the AAPI fraternity to advocate for more patient-centered care.
After inaugurating the Convention with traditional prayers and blessings by Hindu Priests, Congressman Buddy Carter, representing the 1st District in Georgia, said, “If there is anything that the COVID-19 pandemic laid bare it is that our country is too dependent on foreign sources of critical pharmaceutical and medical supplies. I reintroduced bipartisan, bicameral legislation to retake control of America’s health care supply chain. For America’s national security, the legislation incentivizes the domestic manufacturing of drugs and other medical supplies to make the U.S. supply chain less dependent on foreign countries like China.” The only pharmacist in the US Congress, Rep. Carter referred to how the middlemen hike up the prize of drugs by upto 47% in the US, and urged the AAPI fraternity to advocate for more patient-centered care. Dr. Kulkarni spoke about the many programs and plans offered by the Government of India to alleviate the sufferings of the people of India during the pandemic. Dr. Kulkarni stressed the importance of Indo-US Strategic Alliance, especially in the health sector, while pointing out India’s contributions providing the world with quality drugs for cheaper prizes.
Dr. Kulkarni spoke about the many programs and plans offered by the Government of India to alleviate the sufferings of the people of India during the pandemic. Dr. Kulkarni stressed the importance of Indo-US Strategic Alliance, especially in the health sector, while pointing out India’s contributions providing the world with quality drugs for cheaper prizes.
 The Women’s Forum led by Drs. Anjana Samadhar, Uma Jonnalagadda, and Udaya Shivangi featured eminent women leaders, including Keisha Lance Bottoms, Mayor of Atlanta, Dr. Swati Kulkarni, India’s Consular General in Atlanta, Prof. Amita Sehgal, Professor of Neuroscience at UPENN, Dr. Nahid Bhadella, Director of Center for Emerging Infectious Diseases Policy & Reasearch; and, Dr. Mona Khanna, Emmy Award Winning Journalist.
The Women’s Forum led by Drs. Anjana Samadhar, Uma Jonnalagadda, and Udaya Shivangi featured eminent women leaders, including Keisha Lance Bottoms, Mayor of Atlanta, Dr. Swati Kulkarni, India’s Consular General in Atlanta, Prof. Amita Sehgal, Professor of Neuroscience at UPENN, Dr. Nahid Bhadella, Director of Center for Emerging Infectious Diseases Policy & Reasearch; and, Dr. Mona Khanna, Emmy Award Winning Journalist. Her advice for younger generation if they want to follow her, Sherawat said, “If you want to be an actress, I would say, start with your dance training and relaxing training.”
Her advice for younger generation if they want to follow her, Sherawat said, “If you want to be an actress, I would say, start with your dance training and relaxing training.” During the nearly 2 hours long live performance. She showcased the influences of her Indian-American heritage to create music that is refreshingly unique and contemporary, seamlessly fusing together the intricacies of Indian music with elements of electronic and hip-hop for an undeniably catchy sound.
During the nearly 2 hours long live performance. She showcased the influences of her Indian-American heritage to create music that is refreshingly unique and contemporary, seamlessly fusing together the intricacies of Indian music with elements of electronic and hip-hop for an undeniably catchy sound. Known to be a leading ethnic medical organization that represents nearly 100,000 physicians and fellows of Indian Origin in the US, and being their voice and providing a forum to its members to collectively work together to meet their diverse needs, AAPI members are proud to contribute to the wellbeing of their motherland India and their adopted land, the United States. The convention is forum to network, share knowledge and thoughts, and thus, enrich one another, and rededicate ourselves for the health and wellbeing of all peoples of the world. For more details, please visit:
Known to be a leading ethnic medical organization that represents nearly 100,000 physicians and fellows of Indian Origin in the US, and being their voice and providing a forum to its members to collectively work together to meet their diverse needs, AAPI members are proud to contribute to the wellbeing of their motherland India and their adopted land, the United States. The convention is forum to network, share knowledge and thoughts, and thus, enrich one another, and rededicate ourselves for the health and wellbeing of all peoples of the world. For more details, please visit: 
 After graduating with distinction from Kakatiya Medical College, NTR University of Health Sciences in India, she did Residency at University of Miami & University of Illinois, and Fellowship in Pediatric Anesthesiology at University of Michigan.Narrating her childhood ambitions “my parents always encouraged and nurtured me the skills to be a leader and this positive culture influenced me throughout my childhood,” recalls Dr. Gotimukula, who grew up in a family of engineers at Regional Engineering College Campus all her childhood. Her ambition in childhood was “to become a doctor, both to make her parents happy, and to do good for the community. Joining medical school and later on, practicing Medicine was a dream come true and says “I am thankful to my parents and my family who motivated me and mentored me to achieve my goals.”
After graduating with distinction from Kakatiya Medical College, NTR University of Health Sciences in India, she did Residency at University of Miami & University of Illinois, and Fellowship in Pediatric Anesthesiology at University of Michigan.Narrating her childhood ambitions “my parents always encouraged and nurtured me the skills to be a leader and this positive culture influenced me throughout my childhood,” recalls Dr. Gotimukula, who grew up in a family of engineers at Regional Engineering College Campus all her childhood. Her ambition in childhood was “to become a doctor, both to make her parents happy, and to do good for the community. Joining medical school and later on, practicing Medicine was a dream come true and says “I am thankful to my parents and my family who motivated me and mentored me to achieve my goals.” As the President of AAPI, Dr. Gotimukula will work towards “strengthening the organization’s mission, encourage participation of more young physicians, develop the best communications platforms for Indian American Physicians and keep the members well connected. “Patience, Perseverance, Passion and Positive Attitude,” are her mantra to be successful in leadership. She realizes that leadership is a skill and these attributes within her have been well recognized by the physician community locally and nationally.
As the President of AAPI, Dr. Gotimukula will work towards “strengthening the organization’s mission, encourage participation of more young physicians, develop the best communications platforms for Indian American Physicians and keep the members well connected. “Patience, Perseverance, Passion and Positive Attitude,” are her mantra to be successful in leadership. She realizes that leadership is a skill and these attributes within her have been well recognized by the physician community locally and nationally.
 As a woman leader and as the elected leader of a diverse organization such as AAPI, Dr. Gotimukula is aware of the many challenges she is likely to encounter as AAPI’s President. “As leader of the largest physician ethnic nonprofit organization with diverse cultures, yes, challenges are expected.” “On a personal note, time management, balancing career and family responsibilities,” will be challenging. Dr. Gotimukula plans to address them with proper communication, nurture team and engage BK members in problem solving. Being an anesthesiologist, profession has taught me the skills of multi-tasking and staying focused! Daily Meditation and physical exercise keep me energetic and productive until the last minute of my day. Being a woman, I have leaned into being compassionate, empathetic, persevering, patient, and resilient.
As a woman leader and as the elected leader of a diverse organization such as AAPI, Dr. Gotimukula is aware of the many challenges she is likely to encounter as AAPI’s President. “As leader of the largest physician ethnic nonprofit organization with diverse cultures, yes, challenges are expected.” “On a personal note, time management, balancing career and family responsibilities,” will be challenging. Dr. Gotimukula plans to address them with proper communication, nurture team and engage BK members in problem solving. Being an anesthesiologist, profession has taught me the skills of multi-tasking and staying focused! Daily Meditation and physical exercise keep me energetic and productive until the last minute of my day. Being a woman, I have leaned into being compassionate, empathetic, persevering, patient, and resilient.

 Her biggest achievement in life so far is “Being what I am today, a physician, a leader, and a humble human being and be able to give back to my society,” says Dr. Gotimukula. Among the goals for AAPI, the visionary woman leader says, “With the collaboration, cooperation and support of the Executive Committee, and the entire AAPI family, I want to build a strong support system to protect the IMG physicians and their issues and help with physician burnout. I will further the existing educational goals and charitable goals and engage member physicians to support these goals.” While dedicating her talents, skills, and experiences for the AAPI family, which she has come to call as her own, Dr. Gotimukula says, “I am looking forward to get the best wishes & blessings from our members in my pursuit to lead this prestigious organization and do the best to our physician community.”
Her biggest achievement in life so far is “Being what I am today, a physician, a leader, and a humble human being and be able to give back to my society,” says Dr. Gotimukula. Among the goals for AAPI, the visionary woman leader says, “With the collaboration, cooperation and support of the Executive Committee, and the entire AAPI family, I want to build a strong support system to protect the IMG physicians and their issues and help with physician burnout. I will further the existing educational goals and charitable goals and engage member physicians to support these goals.” While dedicating her talents, skills, and experiences for the AAPI family, which she has come to call as her own, Dr. Gotimukula says, “I am looking forward to get the best wishes & blessings from our members in my pursuit to lead this prestigious organization and do the best to our physician community.” “Remembering and memorializing the brave AAPI Warriors and thousands of healthcare workers, who have sacrificed their lives at the service of humanity, especially during the Deadly Covid Pandemic is the major theme during the Convention,” said Dr. Sudhakar Jonnalagadda, President of AAPI. “This convention is a tribute to those who have lost their lives and to the frontline medical professionals who are at the forefront, combating the pandemic around the globe,” he added.
“Remembering and memorializing the brave AAPI Warriors and thousands of healthcare workers, who have sacrificed their lives at the service of humanity, especially during the Deadly Covid Pandemic is the major theme during the Convention,” said Dr. Sudhakar Jonnalagadda, President of AAPI. “This convention is a tribute to those who have lost their lives and to the frontline medical professionals who are at the forefront, combating the pandemic around the globe,” he added. The annual convention this year is being organized by AAPI’s Atlanta Chapter, chaired by Dr. Sreeni Gangasani. The inaugural Nite’s Gala was hosted by Georgia Association of Physicians of Indian Origin (GAPI), during which several leaders of GAPI, including Drs. Indrani Indrakrishnan, Raghu Lolabhattu, Manoj Shah, Yogesh Joshi, Arvind Gupta, PB Rao, Dilip Patel, Uma Jonnagalada and Tarun Gosh addressed the audience. In her address, Dr. Indrani Indrakrishnan shared with the audience of GAPI’s educational, philanthropic, humanitarian, political, entertaining and social activities. Educational scholarships were presented to deserving students from the region.
The annual convention this year is being organized by AAPI’s Atlanta Chapter, chaired by Dr. Sreeni Gangasani. The inaugural Nite’s Gala was hosted by Georgia Association of Physicians of Indian Origin (GAPI), during which several leaders of GAPI, including Drs. Indrani Indrakrishnan, Raghu Lolabhattu, Manoj Shah, Yogesh Joshi, Arvind Gupta, PB Rao, Dilip Patel, Uma Jonnagalada and Tarun Gosh addressed the audience. In her address, Dr. Indrani Indrakrishnan shared with the audience of GAPI’s educational, philanthropic, humanitarian, political, entertaining and social activities. Educational scholarships were presented to deserving students from the region. Dr. Kulkarni shared with the audience about the many programs and plans offered by the Government of India to alleviate the sufferings of the people of India during the pandemic. Dr. Kulkarni stressed the importance of Indo-US Strategic Alliance, especially in the health sector, while pointing out India’s contributions providing the world with quality drugs for cheaper prizes. Congresswoman Carolyn Bourdeaux representing the 7th Congressional district of Georgia was introduced to the audience by Dr. Sreeni Gangasani. Sharing her own close association with the South Asian community, Rep. Carolyn Bourdeaux said, her district is home to the largest South Asian population in the South East. “I have so many wonderful friends in this community for many years I have had many friends who are from South Asia,” she said. “I have been in Washington for about 6 months and I have worked very hard to Advocate on behalf of the South Asian Community.”
Dr. Kulkarni shared with the audience about the many programs and plans offered by the Government of India to alleviate the sufferings of the people of India during the pandemic. Dr. Kulkarni stressed the importance of Indo-US Strategic Alliance, especially in the health sector, while pointing out India’s contributions providing the world with quality drugs for cheaper prizes. Congresswoman Carolyn Bourdeaux representing the 7th Congressional district of Georgia was introduced to the audience by Dr. Sreeni Gangasani. Sharing her own close association with the South Asian community, Rep. Carolyn Bourdeaux said, her district is home to the largest South Asian population in the South East. “I have so many wonderful friends in this community for many years I have had many friends who are from South Asia,” she said. “I have been in Washington for about 6 months and I have worked very hard to Advocate on behalf of the South Asian Community.”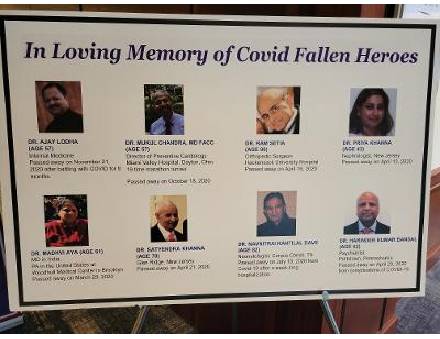 Describing herself as a friend of India and Indian Americans, the Congresswoman said, she is an active member of the India Caucus in the House, she said, “India is a very very important strategic partner to the United States,” and promised to work with the federal government in helping India especially during the pandemic. The inaugural nite’s star attraction was the young and energetic artist Vidya Vox who entertained the audience with song, music and dances. During the nearly 2 hours long live performance. She showcased the influences of her Indian-American heritage to create music that is refreshingly unique and contemporary, seamlessly fusing together the intricacies of Indian music with elements of electronic and hip-hop for an undeniably catchy sound. The delegates were presented with live performances of Bhartanatyam, Thillana and fusion dances by local artists, displaying unique talents in Indian classical dance forms. The popular and much loved Mehfil E Khaas provided AAPI members and families a platform to showcase their talents impromptu, in music, dance, jokes and Shero Shayari in an informal setting.
Describing herself as a friend of India and Indian Americans, the Congresswoman said, she is an active member of the India Caucus in the House, she said, “India is a very very important strategic partner to the United States,” and promised to work with the federal government in helping India especially during the pandemic. The inaugural nite’s star attraction was the young and energetic artist Vidya Vox who entertained the audience with song, music and dances. During the nearly 2 hours long live performance. She showcased the influences of her Indian-American heritage to create music that is refreshingly unique and contemporary, seamlessly fusing together the intricacies of Indian music with elements of electronic and hip-hop for an undeniably catchy sound. The delegates were presented with live performances of Bhartanatyam, Thillana and fusion dances by local artists, displaying unique talents in Indian classical dance forms. The popular and much loved Mehfil E Khaas provided AAPI members and families a platform to showcase their talents impromptu, in music, dance, jokes and Shero Shayari in an informal setting. Physicians of Indian Origin in the United States are reputed to be leading health care providers, holding crucial positions in various hospitals and health care facilities around the nation and the world. Known to be a leading ethnic medical organization that represents nearly 100,000 physicians and fellows of Indian Origin in the US, and being their voice and providing a forum to its members to collectively work together to meet their diverse needs, AAPI members are proud to contribute to the wellbeing of their motherland India and their adopted land, the United States. The convention is forum to network, share knowledge and thoughts, and thus, enrich one another, and rededicate ourselves for the health and wellbeing of all peoples of the world.
Physicians of Indian Origin in the United States are reputed to be leading health care providers, holding crucial positions in various hospitals and health care facilities around the nation and the world. Known to be a leading ethnic medical organization that represents nearly 100,000 physicians and fellows of Indian Origin in the US, and being their voice and providing a forum to its members to collectively work together to meet their diverse needs, AAPI members are proud to contribute to the wellbeing of their motherland India and their adopted land, the United States. The convention is forum to network, share knowledge and thoughts, and thus, enrich one another, and rededicate ourselves for the health and wellbeing of all peoples of the world. Dr. Turner says the research team followed 41 people who received an mRNA vaccine over the course of six months. Of those, 14 participants provided periodic samples of their lymph nodes in order to measure the immune reaction set in to motion by the vaccine. What they found caught them a bit off guard.
Dr. Turner says the research team followed 41 people who received an mRNA vaccine over the course of six months. Of those, 14 participants provided periodic samples of their lymph nodes in order to measure the immune reaction set in to motion by the vaccine. What they found caught them a bit off guard. And even after lymph node activity returns to normal, Dr. Turner says those specially trained cells are likely to remain for years. “We know that these cells can migrate to the bone marrow and persist for decades, generating antibodies,” he said. Dr. Turner says there is still a chance that booster shots could be needed if a variant escapes our immune response.
And even after lymph node activity returns to normal, Dr. Turner says those specially trained cells are likely to remain for years. “We know that these cells can migrate to the bone marrow and persist for decades, generating antibodies,” he said. Dr. Turner says there is still a chance that booster shots could be needed if a variant escapes our immune response. Researchers report that among the women studied:
Researchers report that among the women studied: That’s a surprising position for the country that’s home to the world’s biggest vaccine manufacturer, the
That’s a surprising position for the country that’s home to the world’s biggest vaccine manufacturer, the  On June 21, India administered some
On June 21, India administered some  France, Germany and Italy, among other countries, now advise only one dose of vaccine for people with a healthy immune system and a confirmed previous diagnosis. Many scientists who have studied immune responses to vaccination say such policies are a sensible way to make the most of
France, Germany and Italy, among other countries, now advise only one dose of vaccine for people with a healthy immune system and a confirmed previous diagnosis. Many scientists who have studied immune responses to vaccination say such policies are a sensible way to make the most of  The new vaccination policy, which took considerable prodding and criticism from the Supreme Court before the Centre decided to act, will see the government purchasing 75% of the vaccines produced by the manufacturers and distributing it free to states, based on their population, disease burden and vaccination progress, with the remaining 25% production allocated for private hospitals. However, experts say that India needs to administer a minimum of 1 crore doses a day in order to inoculate its 95-crore strong adult population by December. Moreover, vaccine availability is still patchy. That also explains why over 82% of the doses administered are the first shot.India’s vaccination record has been middling among the world’s 30 most populous countries with a rank 16 among them in terms of doses per 100 population. At 19.6 as of June 19, India’s level is less than a fifth of what the UK has achieved.
The new vaccination policy, which took considerable prodding and criticism from the Supreme Court before the Centre decided to act, will see the government purchasing 75% of the vaccines produced by the manufacturers and distributing it free to states, based on their population, disease burden and vaccination progress, with the remaining 25% production allocated for private hospitals. However, experts say that India needs to administer a minimum of 1 crore doses a day in order to inoculate its 95-crore strong adult population by December. Moreover, vaccine availability is still patchy. That also explains why over 82% of the doses administered are the first shot.India’s vaccination record has been middling among the world’s 30 most populous countries with a rank 16 among them in terms of doses per 100 population. At 19.6 as of June 19, India’s level is less than a fifth of what the UK has achieved. Consul General of India NY Randhir Jaiswal, who briefly attended the event with DCG NY Shatrughan Sinha, appreciated and encouraged the participants.Celebrity yoga instructor, Reiki healer, and health coach Thara Natalie gave yoga lessons for all ages. She also shared health tips during the one-hour session. Singer and song writer Jay Sean was the guest of honor while former Miss America and American public speaker and actress Nina Davuluri, also a yoga practitioner, compered the event.
Consul General of India NY Randhir Jaiswal, who briefly attended the event with DCG NY Shatrughan Sinha, appreciated and encouraged the participants.Celebrity yoga instructor, Reiki healer, and health coach Thara Natalie gave yoga lessons for all ages. She also shared health tips during the one-hour session. Singer and song writer Jay Sean was the guest of honor while former Miss America and American public speaker and actress Nina Davuluri, also a yoga practitioner, compered the event. “Last year was tough for everyone. Now, the community is slowly reeling out of the pandemic. The benefits of yoga are known to the entire world. We hope this event can give a positive push to our attempts to get back to the pre-pandemic days,” said FIA chairman Ankur Vaidya. He expressed his gratitude to CGI NY Jaiswal and DCG Sinha for their continued support in making the Yoga Day celebration a success.FIA provided complimentary coffee, munchkins, water, T-shirt, and yoga mat to all participants in attendance and held an attendee raffle in which 5 Google home devices were raffled as thank-you giveaways to the attendees.
“Last year was tough for everyone. Now, the community is slowly reeling out of the pandemic. The benefits of yoga are known to the entire world. We hope this event can give a positive push to our attempts to get back to the pre-pandemic days,” said FIA chairman Ankur Vaidya. He expressed his gratitude to CGI NY Jaiswal and DCG Sinha for their continued support in making the Yoga Day celebration a success.FIA provided complimentary coffee, munchkins, water, T-shirt, and yoga mat to all participants in attendance and held an attendee raffle in which 5 Google home devices were raffled as thank-you giveaways to the attendees. Prime Minister Narendra Modi launched the mYoga fitness app on the occasion of International Yoga Day. Jointly developed by the Ministry of Ayush and the World Health Organization, the mYoga app aims to bring assisted yoga training to everyone with a smartphone for free without needing any signing in. Check out all you want to know about the new WHO mYoga app, available on both the Google Play Store and Apple App Store. The application is completely free and has no sign up required. Here’s how it works.
Prime Minister Narendra Modi launched the mYoga fitness app on the occasion of International Yoga Day. Jointly developed by the Ministry of Ayush and the World Health Organization, the mYoga app aims to bring assisted yoga training to everyone with a smartphone for free without needing any signing in. Check out all you want to know about the new WHO mYoga app, available on both the Google Play Store and Apple App Store. The application is completely free and has no sign up required. Here’s how it works.
 Asked what he thought about civil rights in India under the current administration there, he told the media, “Democracy cannot just be a word; democracy is about who you care for, your people and education. We are human beings … in jeopardy. I think in India the government is stable but people are poor – too poor… We need to make it right,” Jackson said. Sounding hopeful about working with the Narendra Modi government, he said, “I think the moment we talk [with Modi], we can act together on economic policy and democracy. Modi and I should work together on democracy,” Jackson said. He asked the Indian diaspora to support the poor in India with no homes, work or jobs, saying, “We members of the diaspora are blessed to be in good shape.”
Asked what he thought about civil rights in India under the current administration there, he told the media, “Democracy cannot just be a word; democracy is about who you care for, your people and education. We are human beings … in jeopardy. I think in India the government is stable but people are poor – too poor… We need to make it right,” Jackson said. Sounding hopeful about working with the Narendra Modi government, he said, “I think the moment we talk [with Modi], we can act together on economic policy and democracy. Modi and I should work together on democracy,” Jackson said. He asked the Indian diaspora to support the poor in India with no homes, work or jobs, saying, “We members of the diaspora are blessed to be in good shape.”
 “In the age group of 1-10 years, 3.28 per cent of children contracted COVID-19 infection in the first wave while 3.05 per cent during the second wave. 8.03 per cent were infected in 11-20 years of age group in the first wave and 8.5 per cent in the second wave, ” said Agarwal. He added that prioritising vaccination should be the focus in the country and added that Covid-19 safe behavior should be followed despite low Covid-19 numbers to contain the virulent variants of Coronavirus.
“In the age group of 1-10 years, 3.28 per cent of children contracted COVID-19 infection in the first wave while 3.05 per cent during the second wave. 8.03 per cent were infected in 11-20 years of age group in the first wave and 8.5 per cent in the second wave, ” said Agarwal. He added that prioritising vaccination should be the focus in the country and added that Covid-19 safe behavior should be followed despite low Covid-19 numbers to contain the virulent variants of Coronavirus. The nationwide death rate, however,
The nationwide death rate, however,  We often hear parents complaining about their kids being very aggressive and have rule-breaking behaviour. These kids show anxiety disorders in adolescence. Forgetfulness and low energy level show the deficiency of Vitamin A which is a very crucial group of nutrients. It is also required for a healthy reproductive system in men and women. Green and orange vegetables are a great source of Vitamin A nutrients. For newborn babies, breast milk is considered the best source of vitamin A.
We often hear parents complaining about their kids being very aggressive and have rule-breaking behaviour. These kids show anxiety disorders in adolescence. Forgetfulness and low energy level show the deficiency of Vitamin A which is a very crucial group of nutrients. It is also required for a healthy reproductive system in men and women. Green and orange vegetables are a great source of Vitamin A nutrients. For newborn babies, breast milk is considered the best source of vitamin A. India peaked at adding more than 400,000 cases a day in May, but new infections and deaths have declined across the country since then. There were 85,801 new cases of Covid-19 across India on Monday, the first time fewer than 100,000 infections were added since April 5.The number of coronavirus disease (Covid-19) cases in Delhi reduced further on Monday, dipping below the 300-mark for the first time since March 4. The Capital reported 231 new cases of the viral infection, showed Monday’s health bulletin.
India peaked at adding more than 400,000 cases a day in May, but new infections and deaths have declined across the country since then. There were 85,801 new cases of Covid-19 across India on Monday, the first time fewer than 100,000 infections were added since April 5.The number of coronavirus disease (Covid-19) cases in Delhi reduced further on Monday, dipping below the 300-mark for the first time since March 4. The Capital reported 231 new cases of the viral infection, showed Monday’s health bulletin. Overall, the White House aims to share 80 million doses globally by the end of June, most through COVAX. But 25% of the nation’s excess will be kept in reserve for emergencies and for the U.S. to share directly with allies and partners.“As long as this pandemic is raging anywhere in the world, the American people will still be vulnerable,” Biden said in a statement. “And the United States is committed to bringing the same urgency to international vaccination efforts that we have demonstrated at home.”
Overall, the White House aims to share 80 million doses globally by the end of June, most through COVAX. But 25% of the nation’s excess will be kept in reserve for emergencies and for the U.S. to share directly with allies and partners.“As long as this pandemic is raging anywhere in the world, the American people will still be vulnerable,” Biden said in a statement. “And the United States is committed to bringing the same urgency to international vaccination efforts that we have demonstrated at home.” The annual convention this year is being organized by AAPI’s Atlanta Chapter, chaired by Dr. SreeniGangasani. “The convention team is working hard and over time, to provide a delightful three days of events packed with educational CME credits, world-class entertainment, leadership seminars, networking opportunities, exhibits, and more,” Dr. Gangasani said. “This meeting offers a rich educational and entertainment programs featuring the latest scientific research and advances in clinical practice. In addition, physicians and healthcare professionals from across the country will convene to develop health policy agendas and encourage legislative priorities for the upcoming year.”
The annual convention this year is being organized by AAPI’s Atlanta Chapter, chaired by Dr. SreeniGangasani. “The convention team is working hard and over time, to provide a delightful three days of events packed with educational CME credits, world-class entertainment, leadership seminars, networking opportunities, exhibits, and more,” Dr. Gangasani said. “This meeting offers a rich educational and entertainment programs featuring the latest scientific research and advances in clinical practice. In addition, physicians and healthcare professionals from across the country will convene to develop health policy agendas and encourage legislative priorities for the upcoming year.” Planned to have a limited number of participants due to the ongoing Coivd pandemic and taking into account the safety of those attending, including Physicians, Academicians, Researchers and Medical students, “the annual convention offers extensive academic presentations, recognition of achievements and achievers, and professional networking at the alumni and evening social events,” said Dr. Sajani Shah, Chair of AAPI BOT.
Planned to have a limited number of participants due to the ongoing Coivd pandemic and taking into account the safety of those attending, including Physicians, Academicians, Researchers and Medical students, “the annual convention offers extensive academic presentations, recognition of achievements and achievers, and professional networking at the alumni and evening social events,” said Dr. Sajani Shah, Chair of AAPI BOT. Dr. AnupamaGotimukula, President-Elect of AAPI, said, the delegates at the convention will have Eight Hours of CMEs, coordinated by AAPI CME Chair, Dr. Krishan Kumar, Dr. Vemuri Murthy, Advisor & CME Program Director, and Dr. Sudha Tata, Convention CME Chair, focusing on themes such as how to take care of self and find satisfaction and happiness in the challenging situations they are in, while serving hundreds of patients everyday of their dedicated and noble profession, said Dr. Raghu Lolabhattu, Convention Vice Chair.
Dr. AnupamaGotimukula, President-Elect of AAPI, said, the delegates at the convention will have Eight Hours of CMEs, coordinated by AAPI CME Chair, Dr. Krishan Kumar, Dr. Vemuri Murthy, Advisor & CME Program Director, and Dr. Sudha Tata, Convention CME Chair, focusing on themes such as how to take care of self and find satisfaction and happiness in the challenging situations they are in, while serving hundreds of patients everyday of their dedicated and noble profession, said Dr. Raghu Lolabhattu, Convention Vice Chair. The popular and much loved Mehfil E Khaas will give the AAPI members and families a platform to showcase their talents impromptu, in music, dance, jokes and SheroShayari in an informal setting,” said Dr. Amit Chakrabarty, Secretary of AAPI and coordinator of the Mehfil E Khaas. “Pick up the Mic and you are the Star,” he added. Dr. SatheeshKathula, Treasurer of AAPI said, “The Future of Healthcare” will be discussed at the popular CEO Forum with expert participants from Healthcare, Technological, and Finance industries and moderated by Dr. N. Neealagaru, will share their expertise in ways to establishing and leading successful businesses, healthcare practice, managing investment and creating an ideal lifestyle.
The popular and much loved Mehfil E Khaas will give the AAPI members and families a platform to showcase their talents impromptu, in music, dance, jokes and SheroShayari in an informal setting,” said Dr. Amit Chakrabarty, Secretary of AAPI and coordinator of the Mehfil E Khaas. “Pick up the Mic and you are the Star,” he added. Dr. SatheeshKathula, Treasurer of AAPI said, “The Future of Healthcare” will be discussed at the popular CEO Forum with expert participants from Healthcare, Technological, and Finance industries and moderated by Dr. N. Neealagaru, will share their expertise in ways to establishing and leading successful businesses, healthcare practice, managing investment and creating an ideal lifestyle. The Women’s Forum, led by Drs. AnjanaSamadhar, Uma jonnalagadda, and UdayaShivangi, will feature Ambassador Nikki Haley, Keisha Lance Bottoms, Mayor of Atlanta, Dr. Swati Kulkarni, India’s Consular General in Atlanta, Dr. Susan Bailey, President of American Medical Asociation, Dr. RenuKhator, President & Chancellor of University of Houston; Adv. Sheela Murthy, Founder & President of Murthy Law Form; Prof. Amita Sehgal, Professor of Neuroscience at UPENN, Dr. NahidBhadella, Director of Center for Emerging Infectious Diseases Policy &Reasearch; and, Dr. Mona Khanna, Emmy Award Winning Journalist.
The Women’s Forum, led by Drs. AnjanaSamadhar, Uma jonnalagadda, and UdayaShivangi, will feature Ambassador Nikki Haley, Keisha Lance Bottoms, Mayor of Atlanta, Dr. Swati Kulkarni, India’s Consular General in Atlanta, Dr. Susan Bailey, President of American Medical Asociation, Dr. RenuKhator, President & Chancellor of University of Houston; Adv. Sheela Murthy, Founder & President of Murthy Law Form; Prof. Amita Sehgal, Professor of Neuroscience at UPENN, Dr. NahidBhadella, Director of Center for Emerging Infectious Diseases Policy &Reasearch; and, Dr. Mona Khanna, Emmy Award Winning Journalist. The 25 percent vaccination procurement which was being conducted by the states would now be conducted by the central government, he said, adding that vaccines would be directly purchased by the Centre and given to the states for free.”From June 21, Tuesday, all citizens of India above 18 years of age will be given free vaccination,” Modi added.The Centre, as part of the new vaccination strategy, would procure 75 percent of the vaccines, whereas, the private sector would be allowed to purchase 25 percent of the vaccines, the prime minister said.
The 25 percent vaccination procurement which was being conducted by the states would now be conducted by the central government, he said, adding that vaccines would be directly purchased by the Centre and given to the states for free.”From June 21, Tuesday, all citizens of India above 18 years of age will be given free vaccination,” Modi added.The Centre, as part of the new vaccination strategy, would procure 75 percent of the vaccines, whereas, the private sector would be allowed to purchase 25 percent of the vaccines, the prime minister said. In March 2019, late-stage international trials of aducanumab, involving about 3,000 patients, were halted when analysis showed the drug, given as a monthly infusion, was not better at slowing the deterioration of memory and thinking problems than a dummy drug.But later that year, the US manufacturer Biogen analysed more data and concluded the drug did work, as long as it was given in higher doses. The company also said it significantly slowed cognitive decline.Aducanumab targets amyloid, a protein that forms abnormal clumps in the brains of people with Alzheimer’s that can damage cells and trigger dementia, including:
In March 2019, late-stage international trials of aducanumab, involving about 3,000 patients, were halted when analysis showed the drug, given as a monthly infusion, was not better at slowing the deterioration of memory and thinking problems than a dummy drug.But later that year, the US manufacturer Biogen analysed more data and concluded the drug did work, as long as it was given in higher doses. The company also said it significantly slowed cognitive decline.Aducanumab targets amyloid, a protein that forms abnormal clumps in the brains of people with Alzheimer’s that can damage cells and trigger dementia, including: It’s noteworthy that Dr. Kishore has been honored with the Outstanding Editor Award in Renal and Epithelial Physiology Specialty Section of Frontiers in Physiology, a Switzerland-based publication last week. In a message sent to Dr. Kishore, Publishing Development Journal Manager Georgina Harris, Ph.D. at Frontiers in Lausanne, Switzerland, wrote: “As Frontiers in Physiology reaches 10,000 published articles and more than 10 years online, on behalf of our Chief Editors, we are honored to award you the Outstanding Editor Award in Renal and Epithelial Physiology Specialty Section for your strong editorial contribution to Frontiers in Physiology.” Dr. Harris added: “We would like to highlight our outstanding editors and share our gratitude towards your editorial efforts via social media. Thank you for your strong support for the Journal and providing your time and expertise towards our mission to make all science open!”
It’s noteworthy that Dr. Kishore has been honored with the Outstanding Editor Award in Renal and Epithelial Physiology Specialty Section of Frontiers in Physiology, a Switzerland-based publication last week. In a message sent to Dr. Kishore, Publishing Development Journal Manager Georgina Harris, Ph.D. at Frontiers in Lausanne, Switzerland, wrote: “As Frontiers in Physiology reaches 10,000 published articles and more than 10 years online, on behalf of our Chief Editors, we are honored to award you the Outstanding Editor Award in Renal and Epithelial Physiology Specialty Section for your strong editorial contribution to Frontiers in Physiology.” Dr. Harris added: “We would like to highlight our outstanding editors and share our gratitude towards your editorial efforts via social media. Thank you for your strong support for the Journal and providing your time and expertise towards our mission to make all science open!” After directing an internationally recognized kidney research program as a Principal Investigator at the US Department of Veterans Affairs Salt Lake City Health Care System for about 20 years, where he received a Superior Performance Award and
After directing an internationally recognized kidney research program as a Principal Investigator at the US Department of Veterans Affairs Salt Lake City Health Care System for about 20 years, where he received a Superior Performance Award and  In January 2021, Modi declared at a
In January 2021, Modi declared at a  The sudden and abrupt lock down promulgated by Modi even before the 1st wave of the pandemic hit India caused enormous problems for millions of poor. It lies with the upper-middle-class Indians who were last year
The sudden and abrupt lock down promulgated by Modi even before the 1st wave of the pandemic hit India caused enormous problems for millions of poor. It lies with the upper-middle-class Indians who were last year  On April 16th, during the meeting, Governor Reeves welcomed IAICC’s initiative to improve the economic situation in the State. Mr. Kumar appreciated the support of Governor Reeves for IAICC and said the Chamber’s partnership with Mississippi will not only benefit businesses across the State but also the adjoining States. Dr. Kulkarni told Governor Reeves that the delegation was very pleased with the meeting and hoped there will be a positive momentum in terms of economic development in Mississippi. She also said that she is looking forward to IAICC and the Mississippi Development Authority (MDA) to coordinate a plan for Governor Reeves to visit India soon.
On April 16th, during the meeting, Governor Reeves welcomed IAICC’s initiative to improve the economic situation in the State. Mr. Kumar appreciated the support of Governor Reeves for IAICC and said the Chamber’s partnership with Mississippi will not only benefit businesses across the State but also the adjoining States. Dr. Kulkarni told Governor Reeves that the delegation was very pleased with the meeting and hoped there will be a positive momentum in terms of economic development in Mississippi. She also said that she is looking forward to IAICC and the Mississippi Development Authority (MDA) to coordinate a plan for Governor Reeves to visit India soon. Dr. Susan R. Bailey, President of American Medication Association (AMA), who was the Chief Guest and Distinguished speaker at the launch event, inaugurated JAAPI on Wednesday, May 12, 2021 during a solemn virtual ceremony, attended by hundreds of AAPI members and supporters from around the nation.Dr. Susan R. Bailey, while inaugurating JAAPI said, “It’s my pleasure to celebrate the launch of JAAPI. On behalf of AMA we congratulate AAPI for this new initiative, which will be a great source of medical education. We applaud you and looking forward to reading your great contributions in the years to come.”
Dr. Susan R. Bailey, President of American Medication Association (AMA), who was the Chief Guest and Distinguished speaker at the launch event, inaugurated JAAPI on Wednesday, May 12, 2021 during a solemn virtual ceremony, attended by hundreds of AAPI members and supporters from around the nation.Dr. Susan R. Bailey, while inaugurating JAAPI said, “It’s my pleasure to celebrate the launch of JAAPI. On behalf of AMA we congratulate AAPI for this new initiative, which will be a great source of medical education. We applaud you and looking forward to reading your great contributions in the years to come.” “Physician Leadership In Times of Crisis & Transition” was the theme of an hour long CME presented by Dr. Bailey at the conclusion of the JAAPI launch ceremony. The insightful and practically oriented CME was organized by American Association of Physicians of Indian Origin, in affiliation with Chicago Medical Society and in association with Indian American Medical Association of Illinois IAMA (IL.)
“Physician Leadership In Times of Crisis & Transition” was the theme of an hour long CME presented by Dr. Bailey at the conclusion of the JAAPI launch ceremony. The insightful and practically oriented CME was organized by American Association of Physicians of Indian Origin, in affiliation with Chicago Medical Society and in association with Indian American Medical Association of Illinois IAMA (IL.) In light of the CDC guidance, the Pentagon announced on Friday that fully vaccinated Defense Department personnel no longer need to wear masks indoors or outdoors at Defense facilities.The CDC and the Biden administration have faced pressure to ease restrictions on fully vaccinated people — those who are two weeks past their last required COVID-19 vaccine dose — in part to highlight the benefits of getting the shots. The country’s aggressive vaccination campaign has paid off:
In light of the CDC guidance, the Pentagon announced on Friday that fully vaccinated Defense Department personnel no longer need to wear masks indoors or outdoors at Defense facilities.The CDC and the Biden administration have faced pressure to ease restrictions on fully vaccinated people — those who are two weeks past their last required COVID-19 vaccine dose — in part to highlight the benefits of getting the shots. The country’s aggressive vaccination campaign has paid off:  In January, Prime Minister Narendra Modi
In January, Prime Minister Narendra Modi  Last year, Ekal’s successful initiative against covid was based on self-monitoring, self-reliance, education and cooperative-exchanges. It included a wide-spread awareness campaign about the hygiene, social distancing, food distribution, mask-making and restrictive movements. The new offensive has not only incorporated all these steps in the direct-action roadmap, but also, has started a proactive counter campaign against the misinformation about the vaccine, the danger posed by covid and voodoo- treatments. With extensive reach well beyond its footings, Ekal has mobilized tens of thousands of its school teachers for this information campaign. ‘Ekal-Arogya (Health Foundation)’ has established 24-hr Telehealth lifeline (# 011 41236457) for professional medical counselling.
Last year, Ekal’s successful initiative against covid was based on self-monitoring, self-reliance, education and cooperative-exchanges. It included a wide-spread awareness campaign about the hygiene, social distancing, food distribution, mask-making and restrictive movements. The new offensive has not only incorporated all these steps in the direct-action roadmap, but also, has started a proactive counter campaign against the misinformation about the vaccine, the danger posed by covid and voodoo- treatments. With extensive reach well beyond its footings, Ekal has mobilized tens of thousands of its school teachers for this information campaign. ‘Ekal-Arogya (Health Foundation)’ has established 24-hr Telehealth lifeline (# 011 41236457) for professional medical counselling. The findings showed that the chance of death rose between 2016 and 2018 by 7 per cent in hospitals that did not implement the policy, and fell by 11 per cent in hospitals that did implement the policy.The chances of being re-admitted increased by 6 per cent in the comparison hospitals over time, but stayed the same in hospitals that implemented the policy. Between 2016 and 2018, the length of stay fell by 5 per cent in the hospitals that did not implement the policy, and by 9 per cent in hospitals that did.
The findings showed that the chance of death rose between 2016 and 2018 by 7 per cent in hospitals that did not implement the policy, and fell by 11 per cent in hospitals that did implement the policy.The chances of being re-admitted increased by 6 per cent in the comparison hospitals over time, but stayed the same in hospitals that implemented the policy. Between 2016 and 2018, the length of stay fell by 5 per cent in the hospitals that did not implement the policy, and by 9 per cent in hospitals that did. Dexamethasone, an inexpensive corticosteroid, is an older drug that has been found most beneficial in hospitalized patients who require invasive mechanical ventilation. Yet, when given too early in Covid-19, for example, when supplemental oxygen is not required, dexamethasone may be detrimental. Dexamethasone may also be inappropriate for use in patients that have co-morbidities such as obesity and diabetes. Dexamethasone has been used to reduce cellular immune responses and treat patients with acute respiratory distress syndrome (ARDS). It is now repurposed to combat severe symptoms of Covid-19 and is one tool in the Covid-19 treatment armamentarium.
Dexamethasone, an inexpensive corticosteroid, is an older drug that has been found most beneficial in hospitalized patients who require invasive mechanical ventilation. Yet, when given too early in Covid-19, for example, when supplemental oxygen is not required, dexamethasone may be detrimental. Dexamethasone may also be inappropriate for use in patients that have co-morbidities such as obesity and diabetes. Dexamethasone has been used to reduce cellular immune responses and treat patients with acute respiratory distress syndrome (ARDS). It is now repurposed to combat severe symptoms of Covid-19 and is one tool in the Covid-19 treatment armamentarium. the US and back home in India, spearheading numerous initiatives to help, guide and support the people and the physician community in India on ways to combat and overcome the deadly virus.
the US and back home in India, spearheading numerous initiatives to help, guide and support the people and the physician community in India on ways to combat and overcome the deadly virus. In the letters sent to the 100 US Senators, while acknowledging the respect and influence each of them command on Capitol Hill, Dr. Shivangi said, “we seek your strongest effort to convince the White House to permit more vaccine raw material to be released immediately for local vaccine production, as well as increasing all types of assistance, in a catastrophe of such magnitude.”
In the letters sent to the 100 US Senators, while acknowledging the respect and influence each of them command on Capitol Hill, Dr. Shivangi said, “we seek your strongest effort to convince the White House to permit more vaccine raw material to be released immediately for local vaccine production, as well as increasing all types of assistance, in a catastrophe of such magnitude.” “We are continuing to interact with the physicians back in India to answer their questions. AAPI as a group and individual physicians are reaching out almost on a daily basis with doctors on ground in India,” Dr. Ravi Kolli, Vice President of AAPI said, adding that it is in addition to the calls being received from their friends and families back home.
“We are continuing to interact with the physicians back in India to answer their questions. AAPI as a group and individual physicians are reaching out almost on a daily basis with doctors on ground in India,” Dr. Ravi Kolli, Vice President of AAPI said, adding that it is in addition to the calls being received from their friends and families back home.