History was remade in Odisha State, India, on August 1, 2023, when the Honorable Governor Professor Ganeshi Lal inaugurated the Second Mass Community Bystander Cardiopulmonary Resuscitation (CPR) training event at the Kalinga Institute of Industrial Technology Convention Center in Bhubaneswar.
The statewide life-saving project was the vision of the Hon’ble Chief Minister, Mr. Naveen Patnaik, who inaugurated the project in February 2023 at the Kalinga Stadium in Bhubaneswar. The program is guided by the Indo-US Resuscitation Expert from Chicago, Dr. Vemuri S Murthy, Honorary Advisor (CPR), Government of Odisha (Health & Family Welfare) and Adjunct Faculty, Department of Emergency Medicine, University of Illinois College of Medicine, Chicago, Illinois, USA.
About 1100 participants, mostly students from Kalinga Institute, were trained in Hands-only CPR and Automated External Defibrillator (AED) in 8 hours of intense training by Indian Resuscitation Trainers, led by Dr. Maheswar Parvat, Coordinator of Gandhi Alumni American Heart Association Training Center, Hyderabad, Telangana, helped by the volunteers of the Sri Sathya Sai Seva Organizations, Odisha and AIIMS (Bhubaneswar).
Dr. Vemuri Murthy, in an exclusive post-training event interview, outlined the importance of preventive strategies to combat the number one global killer viz, Heart Disease, more prevalent among South Asians, including Indians and the Indian diaspora. He stressed the need to raise community awareness about preventive strategies such as a healthy diet with less fats and carbohydrates, exercise, control of diabetes and high blood pressure, weight reduction, and reducing stress with holistic approaches such as Yoga and Mindfulness Meditation.
In his team meeting with the Honorable President of India, Mrs. Draupadi Murmu, led by Mr. Krishna Kishore Jasthi at the Odisha Raj Bhavan (Bhubaneswar) on July 27, 2023, Dr. Murthy highlighted the importance of Community CPR programs to improve survivals in Sudden Cardiac Arrests. The Honorable President extended her full support to the CPR programs. She also pointed out the high prevalence of Tuberculosis among Odisha Tribals and the importance of Tuberculosis eradication programs.
Dr. Vemuri S Murthy, an Indo-US resuscitation expert, faculty member at the Department of Emergency Medicine at the University of Illinois College of Medicine, Chicago, Illinois, has been appointed by the Government of Odisha as the State “Advisor on Cardiopulmonary Resuscitation” Projects. He is the first ever to be appointed by the Odisha State Government as the Health Advisor from the United States and will be involved with comprehensive Resuscitation- involved State projects.
Heart disease is a major Global Public Health problem. People of Indian Origin are at a four-times greater risk of heart disease than their Western counterparts and have a greater chance of having a heart attack before 50 years of age.
Dr. Murthy hopes the Life Saver Initiative of the Odisha State will also be implemented soon in the rest of the States in India.
Happy Life Yoga, founded by the renowned EMMY Nominated Filmmaker Tirlok Malik, brought waves of laughter and joy to the hearts of Indian American seniors at a simultaneous in-person and online event in Queens, New York. Hosted by India Home in Jamaica Estate, the event was jointly organized by the Indo-American Senior Citizen Center, GOPIO Manhattan, NY chapters, and The Indian Panorama.
Happy Life Yoga, unlike traditional yoga, doesn’t require mats or physical movements. It is a unique blend of Indian philosophy, Ayurveda, and Yoga, focusing on internal movements of joy, laughter, and happiness through conscious laughter, affirmations, gratitude, forgiveness, and simple breathing techniques. The workshop specially catered to senior citizens, providing them with practical tips and techniques to live happier and healthier lives.
“The power of laughter and joy can transform lives, and Happy Life Yoga is the door that leads to a joyful life,” said Tirlok Malik, the driving force behind this holistic approach. “Through our workshops and events, we want to inspire inner transformation and create a community of individuals across all age groups embracing happiness and self-empowerment.”
The event witnessed a packed house filled with roaring laughter and positive energy, as Tirlok Malik shared his expertise and insights. Having previously conducted workshops for frontline workers, corporates, and global communities worldwide, the Happy Life Yoga team has been making a significant impact on people’s lives.
“We are delighted to see the overwhelming response and enthusiasm from the senior citizen community,” said Neha Lohia, the Director of Happiness for Happy Life Yoga. “The journey towards a happier life begins with self-discovery, and that’s exactly what Happy Life Yoga offers. It was such a joy to see the unstoppable laughter in the room.”
The event was graced by brand partners Get Zage, a specialized service for the elderly in NYC, represented by Claudine and Jack Harplen. Team members who are also filmmakers like John Pina, and Bohan Chen were also present at this event helping with the audience interaction, and filming. The media and news friends from various publications and TV stations were also present to witness Tirlok Malik live in action and to cover the event.
Mukund Mehta, President India Home ,Jagdish Patel President Indo -American Senior Cittizen Center of New York ,Pankaj parikh,Vice President Indo-American Citizen of New York ,Ashok Sheth Vice president -Finance Indo -American Senior Citizen Centterr of New york and Dr. Vasundhara Kalasapudi Executive Dirrector India Home , all said Tirlok Malik’s presntaion of Happyy Life Yoga was extraordinary since seniors overwhelming enjoyed it .The Happy Life yoga workshop was unique in many ways . There were burst of laughters along with many useful tips to stay healthy and Happier for Seniors.
Happy Life Yoga has big plans for the future, including workshops for kids, educational institutes, global and NRI communities, and diverse groups of people both physically in New York and worldwide through online sessions. Their upcoming book and updated website will further contribute to spreading laughter and happiness across the globe through thier meaningful and much needed work.
“We invite everyone to join us on this transformative journey,” said Tirlok Malik. “Embrace Happy Life Yoga, and discover the power of living life to the fullest, with joy, purpose, and fulfillment. Oh and you dont need a mat, the only thing that will move is your belly, jawline and your internal state of mind with tons of laughter, that is my promise.”
About Happy Life Yoga: Happy Life Yoga is a holistic and practical approach to living a happier, healthier, and more fulfilled life. Led by the esteemed EMMY Nominated Filmmaker Tirlok Malik, the organization aims to spread joy, laughter, and happiness through a unique blend of Indian philosophy, Ayurveda, and Yoga. Happy Life Yoga offers interactive workshops, engaging lectures, and uplifting events, empowering individuals to embrace happiness, health, and inner transformation. For more information about Happy Life Yoga and upcoming events, please visit www.happylifeyoga.org.
Like few other ancient practices, yoga has shaped the world’s consciousness. Over a quarter of adults in the United States say they can’t function because they are so stressed. As indicated by the World Wellbeing Association, normal mental issues, for example, uneasiness and melancholy expense the world economy US$ 1 trillion yearly. This International Yoga Day, as we mark the second year since a major pandemic, it is high time that we delve deeper into the benefits of yoga for our post-pandemic world, which is dealing with significant shifts in work, wellness, and personal lives.
This Yoga Day is special because Indian Prime Minister Narendra Modi was in New York to celebrate it at the UN Headquarters this year, where he proposed the idea of a dedicated yoga day in 2014.
While Yoga has become well known with an expected 300 million specialists around the world, 34 million in US alone, the famous origination of yoga is many times restricted to ‘asanas’, the actual stances that structure only one of the eight appendages of yoga as per Yoga Sutras of Patanjali. Although the asanas can provide a workout comparable to that of a gym session, comparing yoga to a gym routine would be like comparing a single wave to the ocean.
Pranayama, or breath mindfulness, is another basic appendage that remains closely connected with asanas is in many cases disregarded in Western practices. Breathing methods can pivot crippling medical problems and as per Dr. Andrew Huberman, a neuroscience teacher in Stanford College, changing how you inhale can end pressure in its tracks. He referred to a specific form of pranayama as a “psychological sigh,” which involves taking a shorter inhalation followed by a longer exhalation.
Whether as basic as a mental murmur or as perplexing as the ‘Wim Hof Technique’, which assisted its namesake with enduring outrageous cold and procure a few notices in the Guinness Book, are characteristically attached to our profound and actual prosperity. Yoga stands out because of the harmony between Asana and Pranayama, which gives us a mindful synchronicity that goes far beyond the mat.
Yama and Niyama, the initial two appendages, lay the moral and moral foundation for a yogic way of life. They create a mutually respectful agreement with the outside world, which results in mental clarity, emotional equilibrium, and spiritual awakening. Strangely, the pandemic has pushed us towards these standards. We have reduced our ecological footprint by working from home and commuting less, which is in line with “Ahimsa,” or nonviolence toward our planet. The thoughtfulness time, then again, mirrors ‘Svadhyaya’ or self-study. For sure, the pandemic has pushed us to ponder our lives, rethinking our connections, and reevaluating our work-life reconciliation.
The fifth appendage, Pratyahara, urges us to separate from the computerized over-burden and reconnect with ourselves. Initial five appendages structure the Bahiranga (outer) yoga, which, when dominated, can assist us with taking advantage of inert human potential.
The last three appendages — Dharana, Dhyana, and Samadhi — address Antaranga yoga, the inner part of yoga that takes advantage of the force of the brain. Here, we track down the underlying foundations of care — an idea now far reaching in the West. Care Based Pressure Decrease (MBSR) procedures, broadly perceived for their adequacy in managing pressure and injury, can be followed back to the standards tracked down in these appendages of yoga.
So, what does this all mean for the world after the pandemic? The comprehensive form of yoga provides a path as we shift our focus to health, well-being, and meaningful living. This isn’t just about adaptability or stress help, yet an excursion of self-change that starts with self-restraint, prompting internal harmony, poise, and euphoria.
Dharana and Dhyana can get us in contact with our inward presence, true serenity and inward joy and those manifest remotely as us having ‘chief presence’, which is progressively pursued in our work places. Yoga’s standards of concentration and discipline have even been applied effectively by Indian young people in bringing home the Scripps Spelling Honey bee titles a large number of years because of training that they get from North South Establishment.
Presently, envision the potential if we somehow happened to expand the utilization of these standards to more extensive life difficulties and open doors. An increase in productivity, creativity, and focus as well as a decrease in stress levels and a greater comprehension and acceptance of oneself and others could result from an expanded yoga practice.
As we celebrate Global Yoga Day this year, it merits thinking about how yoga, in its complete structure, has such a huge amount to propose in rethinking our reality. Its range stretches out past the Indian diaspora, who, with their developing presence across worldwide influential positions, have a one of a kind chance to share this all encompassing comprehension of yoga.
The principles and practices of yoga can help leaders establish businesses and communities that are harmonious and sustainable as the focus of leadership shifts from profit as the single bottom line to a triple bottom line that incorporates social and environmental considerations.
Moreover, it’s interesting to take note of the amount of this old insight lines up with the goals of contemporary developments. For instance, the developing accentuation on psychological wellness tracks down a friend in the yoga sutras. The Yama and Niyama tenets are in line with the focus on sustainable living. Careful practices, when thought about other option, are currently at the very front of standard wellbeing discussions. Yoga’s timeless relevance is demonstrated and its role in shaping our collective future is demonstrated in this synergy.
Yoga provides us with a framework for transformation—an opportunity to redefine our relationship with ourselves, others, and the world as a whole—as we navigate the complexities of our post-pandemic reality. Every small step on the yoga path can result in significant inner shifts, whether through mastering a challenging pose or simply observing our breath.
The force of yoga lies not simply in that frame of mind to assist us with contacting our toes yet in aiding us reach inside and contact our actual selves. To draw in with yoga at this level means to set out on an excursion of persistent learning and development, one that can prepare us to explore existence with versatility, elegance, and serenity.
As we keep on investigating the profundities of yoga, we should make sure to praise its extravagance and variety. Whether you’re rehearsing Ashtanga yoga in a New York studio, pondering by the Ganges, or performing Pranayama in your family room, you’re adding to a worldwide embroidery of change.
Thus, on this Worldwide Yoga Day, we should imagine a future where the comprehension of yoga rises above past the asanas. How about we endeavor to embrace its more profound insight in our regular routines. All things considered, a definitive objective of yoga, as portrayed in the Yoga Sutras, is to in any case the vacillations of the brain. In the midst of the variances of our impacting world, that feeling of quietness may very well be the securing force we want.
The Ludhiana-based institution, which played a pivotal role during the Green Revolution to make India surplus in foodgrains by developing high-yielding strains, has bred a new wheat variety with high amylose starch content, known to reduce risks of type-2 diabetes and cardiovascular diseases.
From “quantity” to “quality” and from “food security” to “nutritional security” — this seems to be the new research focus of the Punjab Agricultural University (PAU).
The Ludhiana-based institution, which played a pivotal role during the Green Revolution to make India surplus in foodgrains by developing high-yielding strains, has bred a new wheat variety with high amylose starch content, known to reduce risks of type-2 diabetes and cardiovascular diseases.
Eating chapatis made from this wheat — called PBW RS1, with RS being short for resistant starch — won’t cause an immediate and rapid rise in glucose levels. The high amylose and resistant starch, instead, ensure that glucose is released more slowly into the bloodstream. Being slower to digest also increases a feeling of satiety; a person consuming 4 chapatis from normal wheat would now feel full after having just two.
It has total starch content, almost the same as the 66-70 per cent in other wheat varieties. But it has 30.3 per cent resistant starch content as against only 7.5-10 per cent for other varieties including PBW 550, PBW 725, HD 3086 and PBW 766, show trials conducted by PAU over four years. The other varieties have 56-62 per cent non-resistant starch content which is nearly half (37.1 per cent) in PWB RS1. Similarly, PBW RS1 has 56.63 per cent amylose compared to only 21-22 per cent in other varieties.
“Chapatis and biscuits made from its whole grain flour also have lower glycemic index (a value used to measure how specific foods increase blood sugar levels), which is linked to the decreased digestibility of the starch. So, it can help bring down the prevalence of diet-related diseases, including obesity and diabetes (especially type 2),” said Achla Sharma, principal wheat breeder at PAU, which was rated the country’s top state agricultural university in 2023 as per the National Institute Ranking Framework.
The variety has been developed over a period of 10 years by a team of wheat breeders led by Dr V S Sohu, head, department of plant breeding and genetics. PAU is the first to combine five novel alleles (genes) affecting resistant starch levels for developing this variety.
Earlier, PAU had released two varieties – PBW Zn1 with high zinc content, and PBW1 Chapati whose flour had premium chapati quality that remained fresh for long – on nutritional lines but none had features as PBW RS1.
Sharma noted that millets are considered healthy because they don’t lead to a spike in blood sugar levels. Dieticians even recommend that diabetic and obese persons give up wheat altogether. “But the fact is that both production and consumption of wheat are much higher and not everyone can have millets on a daily basis. Our idea was, therefore, to breed a wheat variety which feels and tastes like normal wheat, but has higher RS and lower glycemic index,” she said.
But PBW RS1 has a significant drawback that might come in the way of its cultivation by farmers. The average grain yield from the variety at PAU’s field trials has been recorded at 43.18 quintals per hectare. This is below Punjab’s average yield of 48 quintals, which has touched 52 quintals in some years with many farmers harvesting 60 quintals or more.
PAU vice-chancellor Dr Satbir Singh Gosal, however, felt that a beginning towards ushering in nutritional security had to be made. He has urged the Punjab government to promote PBW RS1 flour as a product with “high medicinal and nutritional value”. With proper marketing, the wheat could “fetch higher price” from buyers, similar to the premium that millers are paying for basmati paddy over regular parmal varieties.
“Yes, lower productivity is a challenge. But then, PBW RS1 should be identified as a special-trait variety that will be priced high enough to incentivise farmers to grow it. We have pitched the idea for marketing it as a special quality flour to Markfed (the Punjab State Cooperative Supply & Marketing Federation),” Gosal told The Indian Express, adding that PBW RS1 is the country’s first ever improved wheat variety bred for quality, and not just quantity.
Sharma said seeds for the new variety will be made available to farmers in September to enable them sow in the upcoming rabi season. Apart from its nutritional attributes, PBW RS1 is “completely resistant” to yellow rust and “moderately resistant” to brown rust fungal diseases.
“Chapatis and biscuits from its flour taste just like normal wheat. The high amylose/resistant starch content, translating into increased total dietary fibre, would also be advantageous to bakers and food processors. They can produce products without incorporating fibre or additives from other sources to their formulas,” she said.
The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions with the major theme “True and Total Health is the Wellbeing of Mind, Body, and Spirit” concluded at the iconic Marriott Downtown in Philadelphia, PA with the new leadership of AAPI assuming charge under the leadership of Dr. Anjana Samadder on July8th, 2023.
“I am committed to your well-being and dedicated to advancing AAPI’s mission for a brighter future,” Dr. Anjana Samadder, the new President of the American Association of Physicians of Indian Origin (AAPI) declared during her Presidential Inaugural address in Philadelphia, PA.
Along with Dr. Anjana Samadder, Dr. Satheesh Kathula assumed charge as the President-Elect; Dr. Amit Chakrabarthy as the Vice President; Dr. Sumul Raval as the Secretary; Dr. Sreeni Gangasani as the Treasurer; and Dr. Lokesh Edara as the Chair of the Board of Trustees.
A Gastroenterology Specialist in Columbus, OH, Dr. Anjana Samadder is the spouse of AAPI’s past President, Dr. Gautam Samadder. Dr. Anjana Samadder is affiliated with Mount Carmel West and Mount Carmel East and is a winner of the Gastrointestinal Surgery Excellence Award.
The Convention was officially inaugurated with the chanting of the Sanskrit Mantras, seeking blessings from above, Ribbon cutting and lighting of the traditional Lamp by AAPI leaders and distinguished guests on July 7th, 2023 in Philadelphia, the birthplace of US Independence.
Addressing the over 1,000 delegates from around the nation, Dr. Ravi Kolli, Immediate past President of AAPI spoke about the origins of AAOI 41 years ago and how the physicians of Indian origin have been sought after for their excellence in Medicine. “I applaud you and thank you for your support all through the year. And your presence here with your blessing and your goodwill and warm wishes for the successful 41st Ave annual convention here in our brother City of Brotherly Love Philadelphia,” Dr. Kolli said.
“AAPI has a long and illustrious history of 41 years of existence. Started by a few physicians of Indian origin as they started their journey to this land of opportunities, today, they have succeeded beyond anybody’s expectations. And they have been contributing to our communities and our societies in every possible way. And they’re the most respected physicians of any group that we can call. So, we all should be proud of our heritage and our dedication to our patient care and our successful transition from one to another world and being a role model and almost model citizens in the United States,” Dr. Kolli added.
Picture : TheUNN
In his farewell address, Dr. V. Ranga, immediate past Chair of the BOT, “AAPI is stronger and in safer hands. AAPI is an umbrella organization that has nearly 250 local chapters, specialty societies and alumni organizations. For over 40 years, Indian physicians have made significant contributions to health care in this country, not only practicing in inner cities, rural areas and peripheral communities but also at the top medical schools and other academic centers.”
In his keynote address, Shri Venkaiah Naidu, former Vice President of India stressed the importance of giving back to one’s Motherland, Janmabhoomi, one’s native place as way of returning the many blessings one has received. He highlighted the importance of taking care one’s Mother, Janmabhoomi and Motherland. Praising the many initiatives of AAPI, Shri Naidu said, “AAPI’s programs are more centered around addressing the issues related to the stigma of mental illness and the importance of the practices such as meditation, and yoga, which is a connectivity between the body and the mind.”
The unique event served as a platform for the AAPI members to learn and practice the importance of meditation in resolving one’s pressing health concerns and how Ayurveda, Yoga, and Meditations, the ancient traditions of India offer solutions to the most pressing health problems of the world.
“The secret of meditation is in letting go,” Gurudev Sri Sri Ravi Shankar told the gathering, which included AAPI members and their families. “Stress arises when we have too much to do, and not enough energy or time to do it. We can neither change time nor the number of things we need to do. So, the only option is to increase energy levels. And this can be accomplished through yoga, breathing techniques and meditation,” Sri Sri told the delegates. “A happy mind lets you stay calm; make better decisions and improve the overall quality of life,” he told the Doctors, acknowledging that they lead a stressful life. “You live on average ten years less than the patients you treat, as a consequence of the stressful life you lead,” he told them.
In his address, Rep. Shri Thanedar, the 5th member to join the Samosa Caucus in the US House praised the great contributions of the physicians who worked so hard, especially during the Covid, saving millions of lives.” Congressman Thanedar, who has been instrumental in starting the Hindu Caucus in the US House with the intention of eradicating discrimination on the basis of religion or any other means, wowed to “fight for the transformation of the broken immigration system in the US.”
Picture : TheUNN
Mr. Vivek Ramaswamy in his address passionately spoke about the reasons for his Presidential ambitions. Leaving his successful business, the young and talented Ramaswamy said, “I stepped down from my job as a biotech CEO to focus on a different kinds of cancer. Not a biological cancer, but a cultural cancer that threatened to kill that dream that Martin Luther King had 60 years ago, and that tried to kill the dream that allowed me to achieve everything I had in my life You do get ahead in this country, not on the color of your skin, but on the content of your character and your contributions. A dream that says that any child no matter who they are, where their parents came from, or how long their last name is that we still achieve what we want in this country through our own hard work, our own commitment, our own dedication, that’s the American dream.”
Dr. Willie Underwood, American Medical Association Chair-Elect praised the contributions of Indian American physicians. He said, “You have a lot to celebrate today, not just the past 41 years, but all the work that you do everyday to improve the health outcomes of all Americans. While we have differences and divisions throughout this country, one thing we do share is our desire to be physicians that improve health and healthcare outcomes. I know that together, we can lead this nation forward since we have more in common than differences, with one mission and one goal and that is to improve the health and the health care of this nation.”
Dr. Prem Reddy was honored with the Special Presidential Appreciation and Achievement Award for his Leadership, Entrepreneurship, and Philanthropy. Dr. Ranga Reddy, past AAPI President was conferred with the Lifetime Achievement Award. Dr. Manmeet Ahluwalia was the recipient of the AAPI 2023 Most Distinguished Physician Award; AAPI’s 2023 Most Distinguished Service Award was bestowed on Dr. Udaya Shivangi; Dr. Soumya Reddy Neravetla was the recipient of the AAPI’s 2023 Most Distinguished YPS Award; and, AAPI’s 2023 Most Distinguished MSRF Award was given to Mehul Mehra; Mary Shaya, President of J & B Medical was honored with the prestigious AAPI Presidential Humanitarian Award 2023; and, Stephen Shaya, M.D., Managing Director of Akkad Holdings and Executive Servant Leader at J & B Medical was bestowed with the prestigious AAPI Presidential Healthcare Leadership Award 2023.
The convention included CMEs with accredited courses as well as a variety of panel discussions, presentations and a research and poster competition. There were forums for AAPI Young Physicians Group (AAPI YPS) and for AAPI MSRF for medical students, residents and fellows. A nearly sold out Exhibitor Hall included medical and pharmaceutical products, devices and equipment, insurance and tourism, art, and medical and dental practice-related services.
Led by Dr. Sreeni Gangasani, AAPI CME Chair and Dr. Brahma Sharma, AAPI Convention CME Chair, the CME program provided the highest-level scientific sessions for AAPI delegates. In addition, there was the popular parallel track for Lifestyle Medicine, with focus on Mind- Body side, making it a wholesome CME session, giving everyone something that they loved.
The Women’s Forum led by Dr. Udaya Shivangi had an esteemed panel of successful women leaders. The CEO Forum was moderated by Dr. Achintya Moulick and had eminent leaders from the healthcare and technological industries, who shared their insights on saving healthcare cost, the usefulness and limitations in using AI in the healthcare sector and the need for leadership of Indian Americans in larger political world to address the major concerns of the larger population.
Dr. Raghu Lolabhattu, Chair and CEO of the Convention praised the wonderful team who have been planning for months and organizing the event to make the 2023 annual convention a memorable experience. “I’m glad to be serving as the convention chair. We have been working hard to put together an attractive program for our annual get together, educational activity and family enjoyment. We are fortunate to have a dedicated team of convention committee members helping us to make this event truly historic.”
During the convention held from July 6th to 9th, attendees from across the nation got to engage with an impressive lineup of notable speakers and cutting edge medical and scientific information blended within a rich cultural backdrop of authentic Indian cuisine, fashion, yoga and entertainment from top Indian performers. The event also included AAPI’s Got Talent, organized by the AAPI physicians, was an opportunity for the delegates at the convention to participate and compete in a talent show led by Dr. Amit Chakrabarty and Dr. Seema Arora.
The young and rising artists from the Arya School of Dance performed brilliantly showcasing the history of Bollywood films from the 1960s through the present. The grand finale was the performance by the internationally famed artist, Milka Singh. The long day’s events came to a close with Mehfil & Khaas.
One in seven patient encounters in the United States is with a physician of Indian origin. The American Association of Physicians of Indian Origin (AAPI) is the largest ethnic medical organization in the United States, representing over 100,000 physicians of Indian Origin in the United States. “Welcome to you all to the 42nd Annual Mega Convention, the largest ever in the history of AAPI, to be held at the heart of New York City from July 18-22nd, 2023,” said Dr. Anjana Samader, the new President of AAPI. For more information on AAPI and its many programs and activities, please visit: www.aapiconvention.org/www.appiusa.org
Philadelphia, PA: July 12th, 2023: Joseph M. Chalil, MD, MBA, FACHE was honored with the prestigious Presidential Award by the Association of Physicians of Indian Origin (AAPI) during the 41st annual Convention held at the Philadelphia Marriott Downtown on July 8th, 2023.
Dr. Chalil was bestowed with the award in recognition of his Outstanding Leadership and Excellence in Community Service. Dr. Prem Reddy, CEO & Chairman of Prime Health presented the award during the concluding ceremony of the convention in the presence of an audience of over 1,000 during the Annual Convention and Scientific Assembly of AAPI–the largest ethnic organization of physicians in the U.S. Dr. Ravi Kolli, Immediate Past President of AAPI, lauded Dr. Chalil’s leadership and contributions as the Strategic Advisor of AAPI.
Picture : TheUNN
“Connecting to the brand of AAPI and its extensive US Physician network will lead to an increased visibility of pharmaceutical clinical trials here in the USA,” commented Prof. Joseph M. Chalil, MD, MBA, FACHE, an author and the Chief Strategy Officer of the American Association of Physicians of Indian Origin. He is also the Chief Medical Officer of Novo Integrated Sciences, a Nasdaq-listed company that runs hundreds of clinics in North America.
Dr. Chalil is the President of Clinical Consultants International. He serves as the chairman of the health system advisory board, a professor at the college of business, and a member of the NSU MD executive leadership council at Nova Southeastern University in Florida.
A veteran of the U.S. Navy Medical Corps, Dr. Chalil is also board certified in healthcare management, and has been awarded Fellowship by the American College of Healthcare Executives, an international professional society of more than 40,000 healthcare executives who lead hospitals, healthcare systems and other healthcare organizations.
Dr. Chalil holds three US Patents, and his research includes Clinical Trial Management in Cystic Fibrosis, Multiple Myeloma, and publications in American Journal of Respiratory and Critical Care Medicine. He was the recipient of the 2013 Outstanding 50 Asian Americans in Business Award. A Visiting Professor at various universities and board member of various companies, Dr. Chalil is an expert in US Healthcare policy and a strong advocate for patient centered care. The American Association of Cardiologists of Indian Origin (AACIO) honored Dr. Chalil for his achievements in the field of Cardiology in 2013.
His book, “Beyond the Covid-19 pandemic: Envisioning a Better World by Transforming the Future of Healthcare,” is an Amazon Best Seller. In addition, he is the author of several scientific and research papers in international publications and the publisher of “The Universal News Network.”
(Philadelphia, PA—July 9th, 2023) The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions with the major theme “True and Total Health is the Wellbeing of Mind, Body, and Spirit” concluded here at the iconic Marriott Downtown in Philadelphia, PA with the new leadership of AAPI assuming charge under the leadership of Dr. Anjana Samadder.
“I am committed to your well-being and dedicated to advancing AAPI’s mission for a brighter future,” Dr. Anjana Samadder, the new President of the American Association of Physicians of Indian Origin (AAPI) declared during her Presidential Inaugural address on July 8th, 2023 in Philadelphia, PA.
Along with Dr. Anjana Samadder, Dr. Satheesh Kathula assumed charge as the President-Elect; Dr. Amit Chakrabarthy as the Vice President; Dr. Sumul Raval as the Secretary; Dr. Sreeni Gangasani as the Treasurer; and Dr. Lokesh Edara as the Chair of the Board of Trustees.
A Gastroenterology Specialist in Columbus, OH, Dr. Anjana Samadder is the spouse of AAPI’s past President, Dr. Gautam Samadder. Dr. Anjana Samadder is affiliated with Mount Carmel West and Mount Carmel East and is a winner of the Gastrointestinal Surgery Excellence Award.
The Convention was officially inaugurated with the chanting of the Sanskrit Mantras, seeking blessings from above, Ribbon cutting and lighting of the traditional Lamp by AAPI leaders and distinguished guests on July 7th, 2023 in Philadelphia, the birthplace of US Independence.
Addressing the over 1,000 delegates from around the nation, Dr. Ravi Kolli, Immediate past President of AAPI spoke about the origins of AAOI 41 years ago and how the physicians of Indian origin have been sought after for their excellence in Medicine. “I applaud you and thank you for your support all through the year. And your presence here with your blessing and your goodwill and warm wishes for the successful 41st Ave annual convention here in our brother City of Brotherly Love Philadelphia,” Dr. Kolli said.
“AAPI has a long and illustrious history of 41 years of existence. Started by a few physicians of Indian origin as they started their journey to this land of opportunities, today, they have succeeded beyond anybody’s expectations. And they have been contributing to our communities and our societies in every possible way. And they’re the most respected physicians of any group that we can call. So, we all should be proud of our heritage and our dedication to our patient care and our successful transition from one to another world and being a role model and almost model citizens in the United States,” Dr. Kolli added.
In his farewell address, Dr. V. Ranga, immediate past Chair of the BOT, “AAPI is stronger and in safer hands. AAPI is an umbrella organization that has nearly 250 local chapters, specialty societies and alumni organizations. For over 40 years, Indian physicians have made significant contributions to health care in this country, not only practicing in inner cities, rural areas and peripheral communities but also at the top medical schools and other academic centers.”
In his keynote address, Shri Venkaiah Naidu, former Vice President of India stressed the importance of giving back to one’s Motherland, Janmabhoomi, one’s native place as way of returning the many blessings one has received. He highlighted the importance of taking care one’s Mother, Janmabhoomi and Motherland. Praising the many initiatives of AAPI, Shri Naidu said, “AAPI’s programs are more centered around addressing the issues related to the stigma of mental illness and the importance of the practices such as meditation, and yoga, which is a connectivity between the body and the mind.”
The unique event served as a platform for the AAPI members to learn and practice the importance of meditation in resolving one’s pressing health concerns and how Ayurveda, Yoga, and Meditations, the ancient traditions of India offer solutions to the most pressing health problems of the world.
“The secret of meditation is in letting go,” Gurudev Sri Sri Ravi Shankar told the gathering, which included AAPI members and their families. “Stress arises when we have too much to do, and not enough energy or time to do it. We can neither change time nor the number of things we need to do. So, the only option is to increase energy levels. And this can be accomplished through yoga, breathing techniques and meditation,” Sri Sri told the delegates. “A happy mind lets you stay calm; make better decisions and improve the overall quality of life,” he told the Doctors, acknowledging that they lead a stressful life. “You live on average ten years less than the patients you treat, as a consequence of the stressful life you lead,” he told them.
In his address, Rep. Shri Thanedar, the 5th member to join the Samosa Caucus in the US House praised the great contributions of the physicians who worked so hard, especially during the Covid, saving millions of lives.” Congressman Thanedar, who has been instrumental in starting the Hindu Caucus in the US House with the intention of eradicating discrimination on the basis of religion or any other means, wowed to “fight for the transformation of the broken immigration system in the US.”
Mr. Vivek Ramaswamy in his address passionately spoke about the reasons for his Presidential ambitions. Leaving his successful business, the young and talented Ramaswamy said, “I stepped down from my job as a biotech CEO to focus on a different kinds of cancer. Not a biological cancer, but a cultural cancer that threatened to kill that dream that Martin Luther King had 60 years ago, and that tried to kill the dream that allowed me to achieve everything I had in my life You do get ahead in this country, not on the color of your skin, but on the content of your character and your contributions. A dream that says that any child no matter who they are, where their parents came from, or how long their last name is that we still achieve what we want in this country through our own hard work, our own commitment, our own dedication, that’s the American dream.”
Dr. Willie Underwood, American Medical Association Chair-Elect praised the contributions of Indian American physicians. He said, “You have a lot to celebrate today, not just the past 41 years, but all the work that you do everyday to improve the health outcomes of all Americans. While we have differences and divisions throughout this country, one thing we do share is our desire to be physicians that improve health and healthcare outcomes. I know that together, we can lead this nation forward since we have more in common than differences, with one mission and one goal and that is to improve the health and the health care of this nation.”
Dr. Prem Reddy was honored with the Special Presidential Appreciation and Achievement Award for his Leadership, Entrepreneurship, and Philanthropy. Dr. Ranga Reddy, past AAPI President was conferred with the Lifetime Achievement Award. Dr. Manmeet Ahluwalia was the recipient of the AAPI 2023 Most Distinguished Physician Award; AAPI’s 2023 Most Distinguished Service Award was bestowed on Dr. Udaya Shivangi; Dr. Soumya Reddy Neravetla was the recipient of the AAPI’s 2023 Most Distinguished YPS Award; and, AAPI’s 2023 Most Distinguished MSRF Award was given to Mehul Mehra; Mary Shaya, President of J & B Medical was honored with the prestigious AAPI Presidential Humanitarian Award 2023; and, Stephen Shaya, M.D., Managing Director of Akkad Holdings and Executive Servant Leader at J & B Medical was bestowed with the prestigious AAPI Presidential Healthcare Leadership Award 2023.
The convention included CMEs with accredited courses as well as a variety of panel discussions, presentations and a research and poster competition. There were forums for AAPI Young Physicians Group (AAPI YPS) and for AAPI MSRF for medical students, residents and fellows. A nearly sold out Exhibitor Hall included medical and pharmaceutical products, devices and equipment, insurance and tourism, art, and medical and dental practice-related services.
Led by Dr. Sreeni Gangasani, AAPI CME Chair and Dr. Brahma Sharma, AAPI Convention CME Chair, the CME program provided the highest level talks for AAPI delegates. In addition, there was the popular parallel track for Life style Medicine, with focus on Mind- Body side, making it a wholesome CME session, giving everyone something that they loved.
The Women’s Forum led by Dr. Udaya Shivangi had an esteemed panel of successful women leaders. The CEO Forum was moderated by Dr. Achintya Moulick And had eminent leaders from the healthcare and technological industries, who shared their insights on saving healthcare cost, the usefulness and limitations in using AI in the healthcare sector and the need for leadership of Indian Americans in larger political world to address the major concerns of the larger population.
Dr. Raghu Lolabhattu, Chair and CEO of the Convention praised the wonderful team who have been planning for months and organizing the event to make the 2023 annual convention a memorable experience. “I’m glad to be serving as the convention chair. We have been working hard to put together an attractive program for our annual get together, educational activity and family enjoyment. We are fortunate to have a dedicated team of convention committee members helping us to make this event truly historic.”
During the convention held from July 6th to 9th, attendees from across the nation got to engage with an impressive lineup of notable speakers and cutting edge medical and scientific information blended within a rich cultural backdrop of authentic Indian cuisine, fashion, yoga and entertainment from top Indian performers. The event also included AAPI’s Got Talent, organized by the AAPI physicians, was an opportunity for the delegates at the convention to participate and compete in a talent show led by Dr. Amit Chakrabarty and Dr. Seema Jain.
The young and rising artists from the Arya School of Dance performed brilliantly showcasing the history of Bollywood films from the 1960s through the present. The grand finale was the performance by the internationally famed artist, Milka Singh. The long day’s event came to a close with Mehfil & Khaas.
One in seven patient encounters in the United States is with a physician of Indian origin. The American Association of Physicians of Indian Origin (AAPI) is the largest ethnic medical organization in the United States, representing over 100,000 physicians of Indian Origin in the United States. “Welcome to you all to the 42nd Annual Mega Convention, the largest ever in the history of AAPI, to be held at the heart of New York City from July 18-22nd, 2023,” said Dr. Anjana Samader, the new President of AAPI. For more information on AAPI and its many programs and activities, please visit: www.aapiconvention.org/www.appiusa.org
“I am committed to your well-being and dedicated to advancing AAPI’s mission for a brighter future,” Dr. Anjana Samadder, the new President of the American Association of Physicians of Indian Origin (AAPI) declared during her Presidential Inaugural address on July 8th, 2023 in Philadelphia, PA.
Dr. Anjana Samadder is a Gastroenterology Specialist in Columbus, OH. She is affiliated with Mount Carmel West and Mount Carmel East and is a winner of the Gastrointestinal Surgery Excellence Award. Her husband, Dr. Gautam Samadder is a past President of AAPI.
Along with her, Dr. Satheesh Kathula was administered the oath of office as the President-Elect; Dr. Amit Chakrabarthy as the Vice President; Dr. Sumul Raval as the Secretary; Dr. Sreeni Gangasani as the Treasurer; and Dr. Lokesh Edara as the Chair of the Board of Trustees.
As the President of AAPI, Dr. Samadder says, “I bring a wealth of experience, a visionary perspective, and a deep commitment to serving our community.” According to Dr. Sammader, “The opportunity to make a significant impact and contribute to positive change on a larger scale is what motivates me to embrace a leadership role within AAPI.”
Sharing her vision for AAPI, Dr. Samadder said, “It is to foster improved access to healthcare, promote diversity and inclusion, and amplify the collective voice of our community. Members will always find me by their side. We will collectively always be available to our members’ needs and wellbeing.”
Describing herself as “a dedicated, resilient, passionate, and a determined person, who strives to make a positive impact,” Dr. Sammader said, “Growing up as a child, I always stood up against any injustice, wrongdoing and bullying. My father, a Barrister from the London School of Economics and Political Science always taught us to stand up for ourselves and brought us up with the teaching that women were stronger and better multitaskers, and they are capable of achieving greater heights.”
As a child, young Anjana “was filled with curiosity and an unwavering ambition to create change. My family has been a pillar of support, nurturing my dreams and encouraging me every step of the way.” Dr. Samadder’s inspiration for engaging in philanthropic activities stems from her deep-rooted desire to improve the lives of people in both India and the US. “Witnessing the resilience and strength of individuals facing challenges has been a driving force for me,” she said.
According to Dr. Samadder, “My journey with AAPI in the past 20 years taught me lots of lessons, skills and molded me to take more responsibility in the organization. I will bring to the organization the level of commitment, hard work, experience and skill set needed to accomplish the various goals for AAPI and its members.” Her vision for AAPI is “to help build an ethically strong, morally straight and fiscally responsible organization. It is also vitally important to bring much needed diversity to keep AAPI thriving.”
Over the years, Dr. Samadder has shown great leadership qualities which she proved during her tenure as local chapter President (Central Ohio), Regional Director (Ohio and Michigan) and as AAPI National Treasurer. She has also served diligently in different capacities within AAPI including being National Coordinator for AAPI Annual Convention, 2018 in Columbus. Dr. Smaddar served as the Chair, AAPI Women’s Forum and has organized first live conference of this year in Tampa, Florida (March 19 to 21,2021) with great success. Her vision for AAPI is “to help build an ethically strong, morally straight and fiscally responsible organization. It is also vitally important to bring much-needed diversity to keep AAPI thriving.”
Dr. Anjana Samadder was admitted with Covid for 65 days in the hospital. The coronavirus nearly killed her, but she now has a message to share. “They said you were not supposed to live,” said Dr. Samadder. But she does live. And she wants others to know they can too. “If you have a will, I’m telling you, you can make it. There’s always hope. Never give up. It’s just an ‘I will’ do it kind of a thing,” she said.
“My ordeal with covid -19 was hard, but it also made me strong, resilient and tenacious. My “Never give Up ” attitude kept me going, and now I am ready to hit the ground and work my heart out for our AAPI organization.”
Recalling her fight with the deadly Covid, Dr. Samadder said, “One of my proudest achievements is surviving my near-death experience. Life does not give anyone a second chance, but I did get one after contracting Covid-19 and Cardiac Arrest. This has given me a lot of strength to stand up against all odds.”
Dr. Samadder acknowledged that any time one wants to make any changes, one will face some oppositions. “I plan to address them through strategic planning, inclusive decision-making, and the collective efforts of our dedicated members. Discussions and reasoning and answering questions will help resolve any doubts that may be harbored.”
Realizing that there are challenges and divisions in AAPI, Dr. Sammader is determined to “unify and keep AAPI united through effective communication, fostering collaboration, and actively engaging with our members at all levels. I will strongly stand up against any act that will fragment our organization.”
Amidst loud chores from the audience, Dr. Samadder promised that she is committed to “carry on the existing good work that has been started by our prior AAPI leaders. In addition, I would like to address health care practice issues facing our members both in private practice and in academia. We are working out several other academic, social, and community programs which will help our organization grow. I want to get AAPI represented in US National Health Care Committee by organizing strong lobbying efforts. I will also address physician burnout and establish networking platform for young physicians. I will be open to suggestions from members in order to make our organization one of the strongest ethnic organizations in USA.”
Dr Anjana Samadder said, “AAPI has been at the forefront of Indian physicians’ struggle in procuring front-seat in the American medical fraternity. I assure you that I will continue to carry the torch forward. I will leave no stone unturned to take the AAPI to the glorious heights.” Dr Anjana added that “We, at AAPI, are a large extended family. I look forward to creasing the existing issues, besides bringing about reforms to further enhance the prestige that the AAPI
The Columbus AAPI Convention team has echoed her sentiments, It said, “We have personally known and worked closely with Dr. Anjana Samadder. She has great leadership qualities which she proved during her tenure as local chapter President (Central Ohio), Regional Director (Ohio and Michigan) and as AAPI National Treasurer. She has also served diligently in different capacities within AAPI including being National Coordinator for AAPI Annual Convention, 2018 in Columbus.
Describing her mission in life, Dr. Samadder said, “My life’s mission is to bring about lasting changes and enhance the well-being of individuals and communities. My goals are to stand up for all my beloved AAPI colleagues and to work for a place for AAPI in the National Health Care Committee. I will bring to the organization the level of commitment, hard work, experience and skill set needed to accomplish the various goals for AAPI and its members. I have made a commitment to our members, and I intend to use our platform to make AAPI reach newer heights.”
One in seven patient encounters in the United States is with a physician of Indian origin. The American Association of Physicians of Indian Origin (AAPI) is the largest ethnic medical organization in the United States, representing over 100,000 physicians of Indian Origin in the United States. For more information on AAPI and its many programs and activities, please visit: www.appiusa.org
(Philadelphia, PA—July 8th, 2023) The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions was officially inaugurated with the chanting of the Sanskrit Mantras, seeking blessings from above, Ribbon cutting and lighting of the traditional Lamp by AAPI leaders and distinguished guests on July 7th, 2023 at the famous Philadelphia Marriott Downtown in Philadelphia, the birthplace of US Independence.
Addressing the over 1,000 delegates from around the nation, Dr. Ravi Kolli, President of AAPI in his welcome address, said, “Welcome to Philadelphia for our convention. I applaud you and thank you for your support all through the year. And your presence here with your blessing and your goodwill and warm wishes for the successful 41st Ave annual convention here in our brother City of Brotherly Love Philadelphia.”
While describing the origins of AAPI, 41 years ago and how the physicians of Indian origin have been sought after for their excellence in Medicine, Dr. Kolli said: “AAPI has a long and illustrious history of 41 years of existence. Started by a few physicians of Indian origin as they started their journey to this land of opportunities, today, they have succeeded beyond anybody’s expectations. And they have been contributing to our communities and our societies in every possible way. And they’re the most respected physicians of any group that we can call. So, we all should be proud of our heritage and our dedication to our patient care and our successful transition from one to another world and being a role model and almost model citizens in the United States,” Dr. Kolli added.
In his keynote address, Shri Venkaiah Naidu, former Vice President of India stressed the importance of the need for changes in lifestyle for a healthy living. He urged AAPI members to give back to thier Motherland, Janmabhoomi, their native place as way of returning the many blessings they have received. He highlighted the importance of taking care one’s Mother, Janmabhoomi and Motherland. Praising the many initiatives of AAPI, Shri Naidu said, “AAPI’s programs are more centered around addressing the issues related to the stigma of mental illness and the importance of the practices such as meditation, and yoga, which is a connectivity between the body and the mind.”
In his address, Rep. Shri Thanedar, the 5th member to join the Samosa Caucus in the US House praised the great contributions of the physicians who worked so hard, especially during the Covid, saving millions of lives.” Congressman Thanedar, who has been instrumental in starting the Hindu Caucus in the US House with the intention of eradicating discrimination on the basis of religion or any other means, wowed to “fight for the transformation of the broken immigration system in the US.”
Mr. Vivek Ramaswamy in his address passionately spoke about the reasons for his Presidential ambitions. Leaving his successful business, young and talented Ramaswamy said, “I stepped down from my job as a biotech CEO to focus on a different kinds of cancer. Not a biological cancer, but a cultural cancer that threatened to kill that dream that Martin Luther King had 60 years ago, and that tried to kill the dream that allowed me to achieve everything I had in my life.”
Picture :TheUNN
Ramaswamy quoting Dr. King said, “You do get ahead in this country, not on the color of your skin, but on the content of your character and your contributions. A dream that says that any child no matter who they are, where their parents came from, or how long their last name is that we still achieve what we want in this country through our own hard work, our own commitment, our own dedication, that’s the American dream.”
Dr. Willie Underwood, American Medical Association Chair-Elect praised the contributions of Indian American physicians. He said, “You have a lot to celebrate today, not just the past 41 years, but all the work that you do everyday to improve the health outcomes of all Americans. While we have differences and divisions throughout this country, one thing we do share is our desire to be physicians that improve health and healthcare outcomes. I know that together, we can lead this nation forward since we have more in common than differences, with one mission and one goal and that is to improve the health and the health care of this nation.”
Dr. Prem Reddy was honored with the Special Presidential Appreciation and Achievement Award for his Leadership, Entrepreneurship, and Philanthropy. Dr. Ranga Reddy, past AAPI President was conferred with the Lifetime Achievement Award. Dr. Manmeet Ahluwalia was the recipient of the AAPI 2023 Most Distinguished Physician Award; AAPI’s 2023 Most Distinguished Service Award was bestowed on Dr. Udaya Shivangi; Dr. Soumya Reddy Neravetla was the recipient of the AAPI’s 2023 Most Distinguished YPS Award; and, AAPI’s 2023 Most Distinguished MSRF Award was given to Mehul Mehra, Dr. Kolli said.
Dr. Raghu Lolabhattu, Chair and CEO of the Convention praised the wonderful team who have been planning for months and organizing the event to make the 2023 annual convention a memorable experience. “I’m glad to be serving as the convention chair. We have been working hard to put together an attractive program for our annual get together, educational activity and family enjoyment. We are fortunate to have a dedicated team of convention committee members helping us to make this event truly historic.”
The evening had a Fashion Show by AAPI members, who delighted the audience with their talents and elegant performance. The young and rising artists from the Arya School of Dance performed brilliantly showcasing the history of Bollywood films from the 1960s through the present. The long day’s event came to a close with Mehfil & Khaas. For more information on AAPI and its many programs and activities, please visit: www.aapiconvention.org
(Philadelphia, PA—July 7th, 2023) The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions began on July 6th, 2023 at the famous Philadelphia Marriott Downtown in Philadelphia, the birthplace of US Independence.
Attended by over 500 delegates from around the nation, the coming together of esteemed physicians and their families offers an exciting venue to interact with leading physicians, healthcare professionals, academicians, and scientists of Indian origin from across the country, participating in the scholarly exchange of medical advances, developing health policy agendas, and encouraging legislative priorities in the coming year.
Dr. Ravi Kolli, President of AAPI delivering welcome address
In his welcome address, Dr. Ravi Kolli, President of AAPI said, “It is with immense pleasure that I welcome you all to the 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions. The convention provides a forum for members to facilitate and enable physicians to help excel inpatient care, teaching and research, and to pursue their aspirations in professional and community affairs, by providing opportunities for business partnerships and relationships and to celebrate, coordinate and communicate.”
Dr. Raghu Lolabhattu, Chair and ECO of the Convention praised the wonderful team who have been planning for months and organizing the event to make the 2023 annual convention a memorable experience. “We have been working hard to put together an attractive program for our annual get together, educational activity and family enjoyment. We are fortunate to have a dedicated team of convention committee members helping us to make this event truly historic.”
While introducing Congressman Shri Thanedar, Dr. Sreeni Ganagsani, incoming Treasurer of AAPI and Chair of CME Committee, said, “Shri Thanedar proudly represents the people of Michigan’s 13th Congressional District. Congressman Thanedar is passionate about fighting to improve the lives of hard-working families across the United States.”
In his keynote address, Rep. Thanedar, the 5th member to join the Samosa Caucus in the US House shared with the audience about his humble beginnings in India and how his application to come to the United States to pursue Doctoral Degree was denied four times by the Indian Consulate in Mumbai. “Today, I am proud to state that I had the honor of escorting the Prime Minister of India to deliver his address to the joint session of the US Congress.”
Shri Thandedar delivering keynote address ion the inaugural nite of the 41st AAPI Convention
Born into a large family in Southern India, he knows firsthand the struggles and stigma of poverty, and I had started working as a janitor to meet the needs of my family. “That’s why he’s committed to fighting for more education and job training resources for southeast Michigan, a higher minimum wage, universal health care, and programs to jumpstart entrepreneurship in historically disenfranchised communities. Together, these initiatives will close the racial wealth gap and help more families in the United States,” he said.
Thanedar praised the great contributions of the physicians who worked so hard, especially during the Covid, saving millions of lives.” Congressman Thanedar, who has been instrumental in starting the Hindu Caucus in the US House with the intention of eradicating discrimination on the basis of religion or any other means, wowed to “fight for the transformation of the broken immigration system in the US.”
A section of the audience at the inaugural gala
In his remarks on the great philanthropic activitirs carried out throuthg the Heart to Heart Foundation, Dr. Sunny Anand said, “We’ve been going to villages trying to deliver medical care, and it’s been a journey of more than 50 years. Within the last 10 years, we have set up 10 hospitals where there is no cash counter there is no billing department. All the care is given totally free of course. Our Foundation has touched the lives of so many with more than 220,000 consultations 26,000 heart surgeries or cat interventions completely free of cost. And we are now talking to you about rural Medical College. Come join us in our endeavor to touch many more lives and transform the lives of the rural poor.”
The Regional Directors of AAPI were recognized for their leadership and commitment to the mission o0f AAPI with a plaque presented by Shri Thanedar to each of them.
The entertainment sessions of the inaugural night kickstarted with the “AAPI’s Got Talent contest” where AAPI members showcased their hidden talents. The highly sought after event was led by Dr. Amit Chakrabarty, the incoming Vice President of AAPI and Dr. Seema Arora, past Chair of AAPI BOT. Other cultural programs for the evening included, Bishakh Jyoti Live, Garba and Mehfil & Khaas.
For more information on AAPI and its many programs and activities, please visit: www.aapiconvention.org
The MIT group needed to check whether they could expand that finding into domains all the more usually connected with inventiveness, for example, narrating. They also wanted to find out if they could control what people’s dreams contained and how that controlled content might affect the creative process.
“One of the objectives of our gathering is to give individuals more bits of knowledge into how their mind functions, and furthermore what their mental state is and the way that they might have the option to impact it,” Maes says.
Toward that end, Horowitz worked with a group of individual MIT Media Lab understudies in fostering a gadget called Dormio that could be utilized for designated dream brooding. Changes in muscle tone, heart rate, and skin conductance are three physiological sleep markers that are measured by the glove and sent to an app for a smartphone or laptop.
As somebody wearing the glove enters the N1 express, the application prompts them to dream about a particular point. When the wearer enters the next stage of sleep after a few minutes, the app wakes them up, asks them to describe their dream, and records their response.
According to Esfahany, who is majoring in computation and cognition, a program offered jointly by MIT’s departments of Brain and Cognitive Science and of Electrical Engineering and Computer Science, “Before that device, there were no causal studies where people could guide dreams toward certain topics and then look at post-sleep behavior.”
In a 2020 paper, the researchers first demonstrated that they could utilize the Dormio device for targeted dream incubation. In their new review, they utilized this way to deal with investigate how dreaming, and designated dreaming specifically, impacts imagination.
In a 2020 paper, the researchers first demonstrated that they could utilize the Dormio device for targeted dream incubation. They used this strategy to investigate how creativity is influenced by dreaming, and specifically by targeted dreaming, in their new study.
The researchers divided 49 participants into four groups for this study. One group was given 45 minutes to sleep while the Dormio device asked them to dream of a tree and recorded their dreams. The wearer was again prompted to dream about a tree and encouraged to go back to sleep each time a dream was reported.
A different group of people napped while using the device, but they were only told to watch what they were thinking. Throughout the 45-minute period, two additional groups remained awake: The other was instructed to observe their thoughts, while one of these were given prompts to consider trees.
Subjects were asked to complete three tasks that have previously been shown to correlate with creativity after napping or being awake for 45 minutes. First was a narrating task, where the members were approached to compose an innovative story including “tree.”
Human raters who read the stories and were unaware of which participants were in each group determined that study participants who were instructed to dream about trees produced the most inventive stories. In addition, those who took a break without being prompted to do so displayed greater creativity than those who had remained awake throughout the experiment.
Divergent thinking tasks, two additional measures of creativity, gave the highest scores to those who were instructed to have dreams about trees. In one task, participants were required to think of as many inventive uses for a tree as possible. In the second, individuals were presented with a list of nouns and asked to respond with the first verb that came to mind for each one.
At the point when the specialists broke down each of the three errands, members who snoozed with designated dream brooding performed 43% more imaginatively than members who rested without designated dream hatching, and 78 percent more innovatively than the people who remained alert without brooding.
The scientists likewise found that inside the gathering told to dream about trees, the people who had a bigger number of dreams about trees likewise showed greater imagination in their accounts. These individuals additionally consolidated a large part of the substance of their fantasies in their accounts.
“That proof recommends that it’s not simply being in the N1 rest express that makes individuals more imaginative. According to Esfahany, “people are more creative because they are also utilizing the dreams that are occurring in that sleep state.”
Outfitting the psyche
The analysts likewise found that individuals who rested had the best execution on one more measure connected with inventiveness, known as semantic distance. The difference in meaning between two words or concepts is known as semantic distance. Mother and frog, for instance, would be further apart, while father and mother would be closer together.
The researchers found that people who napped produced word combinations with a much greater semantic distance than those who stayed awake in the verb generation and alternative use tasks. This supports the hypothesis that during rest beginning, the mind unites ideas that it probably won’t interface during waking hours.
“In the event that we guide your reasoning during that period, that amazing chance to look for farther separated ideas is additionally directed,” Esfahany says. ” If we direct you to have a dream about a tree, you’ll develop much broader associations with trees, which you can use to come up with creative responses.
The Dormio device is not required for targeted dream incubation, the researchers emphasize; It can be done with any device that can play and record sound, as well as track sleep. Additionally, they have developed a simpler version of their protocol that is accessible online to anyone who wishes to use it and makes use of a timer rather than tracking sleep states.
“That is actually our objective with a ton of this work: to give individuals more devices to figure out how to bridle their own personalities,” Maes says.
The analysts are presently investigating whether they can grow their fantasy brooding convention to later rest stages, like REM. They are also looking into ways to make the protocol easier to use and use it in other areas, like helping to treat distress caused by nightmares.
When Leo Tolstoy, a Russian philosopher, wrote the opening line of Anna Karenina, he might have been right. Blissful families are indistinguishable; each troubled family is miserable in its own specific manner.”
A new report distributed in Mental Science and drove by a researcher now at the USC Dornsife School of Letters, Expressions and Sciences, recommends that with regards to their cerebrums handling data, individuals who are not forlorn are similar, yet every desolate individual cycles the world in their own, peculiar way.
Overflowing examination shows that forlornness is inconvenient to prosperity and is many times joined by self-announced sensations of not being perceived by others. A new report from the US Top health spokesperson’s office alluded to depression as a general wellbeing emergency in response to the developing number of grown-ups experiencing this condition. Indeed, even before the beginning of the Coronavirus pandemic, around half of U.S. grown-ups revealed encountering quantifiable degrees of depression.
Forlornness is peculiar
While she was a postdoctoral individual at UCLA, Elisa Baek, partner teacher of brain research at USC Dornsife, looked to all the more likely comprehend what adds to such sensations of separation and being misconstrued. Baek and her group utilized a neuroimaging procedure called practical attractive reverberation imaging (fMRI) to look at the cerebrums of 66 first-year understudies while they watched a progression of video cuts. The videos covered a wide range of topics, from melodramatic music videos to party scenes and sporting events, giving researchers a wide range of scenarios to examine.
The UCLA Loneliness Scale, a survey that measures a person’s subjective feelings of loneliness and feelings of social isolation, was given to the participants, whose ages ranged from 18 to 21, prior to being scanned.
In view of the review results, the analysts isolated the members into two gatherings: desolate and “nonlonely” (those not encountering depression). After that, they used fMRI to scan each participant’s brain as they watched the videos.
Contrasting the cerebrum imaging information between the two gatherings, the analysts found that lonelier people displayed more different and eccentric mind handling designs than their non-desolate partners.
This finding is critical in light of the fact that it uncovers that brain comparability, which alludes to how comparable the mind movement examples of various people are, is connected to a common perspective of the world. This common perspective is significant for laying out friendly associations. Individuals who experience the ill effects of depression are not just less like society’s standard of handling the world, yet each desolate individual varies in novel ways, also. The feelings of loneliness and a lack of social connections may be exacerbated by this individuality.
Baek said, “It was amazing for observe that desolate individuals were even less like one another.” The way that they don’t track down shared trait with desolate or nonlonely individuals makes accomplishing social association considerably more challenging for them.
Dejection isn’t tied in with having or not having companions
All in all, does peculiar handling in forlorn people cause dejection, or is it a consequence of depression?
The specialists saw that people with elevated degrees of depression – ; regardless of the number of social connections or friends they had -; were bound to have eccentric cerebrum reactions. This raised the likelihood that being encircled by individuals who see the world uniquely in contrast to oneself might be a gamble factor for depression, regardless of whether one mingles routinely with them.
The study also suggests that a person’s idiosyncratic way of processing the world may be influenced by the degree to which social connections or disconnections change over time.
Looking forward, Baek said she is keen on analyzing individuals who have companions and are socially dynamic yet at the same time feel forlorn. In addition, the researchers are examining how lonely people react to specific situations in different ways. For instance, do desolate individuals show mannerisms while handling unforeseen occasions or questionable social settings in which things can be deciphered in an unexpected way?
Walking 10,000 steps per day has been a benchmark health goal for a while. (Interesting fact: It originated as part of a marketing campaign for an early step counter leading up to the 1964 Tokyo Olympics, and equates to walking about 5 miles). The average American gets far less than this—logging between 3,000 to 4,000 steps each day—and there’s some evidence that upping your daily strides can have some surprising benefits. Here are some of them:
While a brisk stroll may not be as vigorous as high-intensity workouts like running or Spinning, it is an effective way to burn calories and support weight loss. According to a 2018 study published in the journal Obesity, walking 10,000 steps a day is associated with weight loss and management. Plus, it’s a low-impact exercise, making it accessible for all fitness levels. And it elevates your heart rate and activates muscles like your quads, glutes, calves and hamstrings, helping to burn calories and strengthen your lower body.
“Walking is an easy way to increase your calorie burn without your body needing time and energy to recover,” says Rachel MacPherson, CPT, an American Council on Exercise-certified personal trainer with Garage Gym Reviews. “It’s not tiring and won’t cause fatigue on a diet. You can walk a lot during the day without feeling as beat up as you would with higher-intensity cardio. If you add walking to your day, you may find maintaining a healthy weight or losing weight to happen naturally without even noticing.”
Better Mobility
Walking can have a positive impact on your joint health. When you hoof it, your body releases synovial fluid, which acts like engine oil to lubricate your joints and keep them moving smoothly, per a 2019 study published in International Journal of Molecular Sciences. Additionally, a 2021 study found that a regular walking routine helped boost physical performance and reduce knee joint pain in those with arthritis. If you have existing joint pain, engaging in regular low-impact exercise like walking can help relieve pain and prevent joint-related issues in the long run.
“Walking is a natural human movement that improves joint health without the impact of higher-intensity exercises like running, which can aggravate any joint issues you may have,” says MacPherson. “It helps increase circulation and joint fluid, keeping your tissues healthy and moving well.” So while it might be tempting to skip exercise if you have achy joints, walking can truly be beneficial. “When you don’t move enough, your muscles, tendons, and ligaments can become weak or tight in certain areas, especially if you sit a lot,” she adds.
Improved Mood and Brain Function
Engaging in any form of physical activity triggers the release of endorphins—feel-good chemicals that can boost your mood and reduce stress and anxiety. For additional benefits, getting your 10,000 steps outdoors in nature can significantly increase mental health and relieve symptoms of depression and anxiety, according to a 2022 meta-analysis published in theJournal of Clinical Medicine. In addition, 2023 research published in Journal of Alzheimer’s Disease Reportssuggests that regular walking can improve cognitive function and memory.
“Walking 10,000 steps daily will help you feel more focused, sharp, and happier—leading to fewer feelings of physical tension, providing both mental and physical benefits,” says MacPherson.
Speedier Recovery
Research published in Sports Medicine found that engaging in active recovery, or a cool-down, like leisurely walking after intense exercise or strength training can support recovery and promote blood flow to your muscles, helping to prevent muscle stiffness and allow your body to recover faster.
“Active recovery is a more leisurely workout that includes movement that won’t be strenuous enough to cause any further damage to your muscles and won’t require a lot of effort or nutritional demands to perform,” says MacPherson. “Walking 10,000 steps daily can improve your recovery so you are less likely to have sore muscles, and you will perform better during your next workout. Active recovery helps improve the overall recovery process by stimulating blood flow that brings nutrients to the tissues that need it most.”
The Bottom Line
Walking 10,000 steps daily offers a slew of physical and mental health benefits. For example, it can support healthy weight loss, improve joint health, boost mood and brain function and aid recovery. Also, walking is a low-impact exercise that’s accessible to most people. So, if you’re looking for an enjoyable and effective way to improve your fitness level and overall health, lace up those walking shoes and get your steps in! (Originally appeared: EatingWell.com)
Mary Shaya, President of J & B Medical, will be honored with the prestigious American Association of Physicians of Indian Origin (AAPI) Presidential Humanitarian Award 2023. This well-deserved recognition celebrates Ms. Shaya’s exceptional contributions to the Health and Wellness of Americans in need, and her relentless dedication to humanitarian and philanthropic initiatives, which have significantly impacted the lives of American veterans and seniors.
The AAPI Presidential Humanitarian Award 2023 recognizes Ms. Mary Shaya’s exceptional leadership and her relentless pursuit of making a difference in the lives of those in need. Her unwavering commitment to improving the Health and Wellness of Americans has set a benchmark for excellence in the industry.
“On behalf of the American Association of Physicians of Indian Origin (AAPI), it is with great pleasure that I extend my warmest congratulations to you on being selected as the recipient of the AAPI Presidential Humanitarian Award 2023,” said Dr. Ravi Kolli, President of AAPI. “This prestigious award is a testament to your outstanding contributions to the Health and Wellness of Americans in need and your relentless humanitarian and philanthropic initiatives.”
Ms. Shaya’s remarkable achievements will be celebrated at the AAPI Convention 2023, where she will join other esteemed leaders, physicians, and healthcare professionals. The convention provides a platform for sharing knowledge, fostering collaborations, and advancing healthcare practices to benefit individuals across the nation.
Lauding her exceptional leadership, under whom J & B Medical has consistently demonstrated an unwavering commitment to serving the most vulnerable members of the society, particularly veterans and seniors,” Dr. V. Ranga, Chair of AAPI BOT said. “Your organization’s dedication to providing essential healthcare services and support to those in need has had a profound impact on the lives of countless individuals.:
Dr. Anjana Samadder, President-Elect of AAPI said, “Your commitment to enhancing the quality of life for our elderly population is commendable and inspires others in the healthcare industry. The AAPI Presidential Humanitarian Award 2023 is a recognition of your outstanding contributions and the positive impact you have made on the health and well-being of Americans in need.”
Dr. Joseph Chalil, Strategic Advisor of AAPI echoed similar sentiments. “Your tireless efforts in helping veterans and elderly Americans, through various initiatives, have truly made a difference in their lives. Through your leadership, J & B Medical has gone above and beyond to ensure that our nation’s heroes receive the care and assistance they deserve.”
Under the compassionate leadership of Ms. Mary Shaya, J & B Medical has demonstrated exceptional commitment to supporting veterans and elderly individuals in need. Through innovative programs and unwavering dedication, Ms. Shaya has spearheaded initiatives that have positively transformed the lives of those facing various health challenges.
“Your dedication and compassion have not only improved the health outcomes of veterans but also provided them with a renewed sense of hope and well-being. Furthermore, your philanthropic endeavors have touched the lives of American seniors, empowering them to lead healthier and more fulfilling lives. Your leadership, compassion, and unwavering dedication exemplify the values that AAPI stands for, and we are honored to celebrate your achievements.”
Ms. Shaya’s tireless efforts to improve the lives of American veterans have provided them with essential healthcare services and unwavering support. Her initiatives have gone above and beyond to ensure that these esteemed individuals, who have dedicated their lives to serving their country, receive the care and assistance they deserve. Through her visionary leadership, Ms. Shaya has become a beacon of hope, improving countless veterans’ health outcomes and overall well-being.
Ms. Shaya’s philanthropic endeavors have made a profound impact on the lives of American seniors. Her dedication to enhancing the quality of life for elderly individuals has empowered them to lead healthier, more fulfilling lives. Through her unwavering commitment to their well-being, Ms. Shaya has inspired others in the healthcare industry to prioritize the unique needs of seniors, fostering a culture of care and compassion.
American Association of Physicians of India origin (AAPI) was formed 41 years ago and is now the largest ethnic medical organization in the USA representing more than120,000 medicals professional in the USA and is deeply engaged in medical education in India through its mentorship activities with medical students in India and annual Global Healthcare Summit program bring together medical experts and academicians from the USA and India to interact with medical students and postgraduates in India with educational seminars and workshops at the summit. For more information, please visit: www.aapiusa.org
Stephen Shaya, M.D., Managing Director of Akkad Holdings and Executive Servant Leader at J & B Medical, has been chosen to be bestowed with the prestigious American Association of Physicians of Indian Origin (AAPI) Presidential Healthcare Leadership Award 2023. This highly coveted accolade celebrates Dr. Shaya’s outstanding contributions to the future of healthcare delivery and his visionary approach that has propelled innovation and reshaped the healthcare landscape.
Picture : TheUNN
“It is with great pleasure and admiration that I extend my heartfelt congratulations to Stephen Shaya, M.D. on being selected as the recipient of the American Association of Physicians of Indian Origin (“AAPI”) Presidential Healthcare Leadership Award 2023,” said Dr. Ravi Kolli, President of AAPI. “This esteemed accolade recognizes your exceptional contributions to the future of Healthcare Delivery. Your visionary leadership as the Managing Director of Akkad Holdings and Executive Servant Leader at J & B Medical has been instrumental in driving innovation and transforming the healthcare landscape. Your dedication to improving the future of healthcare delivery is an inspiration to all, and we are honored to recognize your remarkable achievements.”
Dr. Shaya’s achievements will be celebrated during the upcoming AAPI Convention in Philadelphia on July 8th, 20203, where he will join other esteemed leaders, physicians, and healthcare professionals worldwide. The convention will provide a platform for sharing knowledge, fostering collaborations, and advancing healthcare practices to benefit patients globally.
The AAPI Presidential Healthcare Leadership Award 2023 is a well-deserved recognition of Dr. Shaya’s exceptional contributions to the future of healthcare delivery. His visionary approach and commitment to innovation have propelled the industry forward and inspired countless healthcare professionals to embrace new possibilities. The prestigious award recognizes Dr. Shaya’s exceptional contributions to the future of healthcare and visionary leadership.
In his congratulatory note, Dr. V. Ranga, Chair of AAPI BOT said, “Your relentless pursuit of excellence and dedication to improving healthcare delivery has left an indelible impact on the industry. Through your visionary approach, you have consistently championed advancements in healthcare technology, research, and patient care.”
Dr. Anajana Samadder, President-Elect of AAPI said, “Your leadership and strategic insights have not only brought about positive change within your organization but have also inspired countless healthcare professionals to embrace innovation and embrace new possibilities. As we celebrate Dr. Shaya’s remarkable achievement, we eagerly anticipate witnessing the continued impact of his visionary leadership on the future of healthcare delivery.”
Dr. Shaya’s relentless pursuit of excellence and unwavering dedication to improving healthcare delivery has impacted the healthcare industry immensely. Through his visionary leadership, he has spearheaded revolutionary initiatives that have transformed healthcare delivery, enhancing patient experiences and outcomes.
Picture : TheUNN
Acknowledging Dr. Shaya’s creative and innovative ways of providing healthcare delivery, Dr. Jospeh Chalil, Strategic Advisor of AAPI said, “Your efforts have not only revolutionized the way healthcare is delivered but have also enhanced the overall patient experience and outcomes. Your commitment to incorporating cutting-edge technologies and fostering collaborations within the industry has set new benchmarks for excellence.:
As Executive Servant Leader of J & B Medical, Dr. Shaya has consistently championed advancements in healthcare technology, research, and patient care. His forward-thinking strategies have reshaped the industry, creating a paradigm shift in how healthcare services are accessed and delivered. By incorporating cutting-edge technologies and fostering collaborations within the field, Dr. Shaya has set new benchmarks for excellence and pushed the boundaries of possibility.
As Managing Director of Akkad Holdings, his family office, his dedication and strategic investments in patient-centered care have revolutionized the healthcare experience. By placing patients at the heart of decision-making, Dr. Shaya has empowered individuals to actively participate in their healthcare journey, fostering a culture of shared responsibility and patient empowerment. His compassionate leadership has improved health outcomes and instilled a renewed sense of hope and well-being among patients.
Dr. Achitya Moulic, Chair of the AAPI CEO Forum at the AAPI Convention 2023, where Dr. Shaya will be a keynote speaker, said, “Your tireless advocacy for patient-centered care has been pivotal in shifting the focus towards holistic and personalized healthcare. By prioritizing patient needs and preferences, you have empowered individuals to actively participate in their own healthcare journey, fostering a culture of shared decision-making and patient empowerment.”
The AAPI Presidential Healthcare Leadership Award 2023 is a well-deserved recognition of Dr. Shaya’s exceptional contributions to the future of healthcare delivery. His visionary approach and commitment to innovation have propelled the industry forward and inspired countless healthcare professionals to embrace new possibilities.
“Dr. Shaya’s accomplishments are a testament to his unwavering commitment to improving healthcare and transforming lives. His visionary leadership and remarkable contributions have set new standards for excellence and inspired the entire healthcare community. As we celebrate Dr. Stephen Shaya’s remarkable achievements, we eagerly anticipate witnessing the continued impact of his visionary leadership on the future of healthcare delivery,” Dr. Kolli added.
American Association of Physicians of India origin (“AAPI”) was formed 41 years ago and is now the largest ethnic medical organization in the USA representing more than 120,000 medicals professional in the USA and is deeply engaged in medical education in India through its mentorship activities with medical students in India and annual Global Healthcare Summit program bring together medical experts and academicians from the USA and India to interact with medical students and postgraduates in India with educational seminars and workshops at the summit. For more information, please visit: www.aapiusa.org
In 2021, Shaheen Aamir found herself too exhausted to engage in active play with her children. She recalls telling them, “‘You guys can play, Mom wants to sit.'” Aamir admits to never exercising and being concerned about her weight at the time.
Fast forward three years, and now 32-year-old Aamir begins each day with yoga or dancing. This transformation occurred after she enrolled in a four-month course focused on preventing Type 2 diabetes. “It changed my life, health- and fitness-wise,” says Aamir, adding that she feels “light and energetic” and has experienced a boost in self-esteem.
Aamir, an immigrant from Pakistan with a family history of diabetes, was among nearly 550 individuals who participated in the South Asian Healthy Lifestyle Intervention Program (SAHELI). The study aimed to address and prevent diabetes and heart disease among South Asians residing in the Chicago area.
Compared to whites, Asian Americans and Pacific Islanders have higher diabetes rates and are more likely to develop Type 2 diabetes at younger ages and lower body weights. South Asians, Filipinos, and Pacific Islanders face particularly high risks among Asian subgroups.
A team of Asian American researchers is working to uncover the reasons behind these disparities and develop programs like SAHELI to reduce diabetes rates. They are investigating root causes and improved solutions while advocating for their communities to adopt healthier habits. Here are some key findings that can make a difference.
Identifying the Dangers of ‘Skinny Fat’
In the mid-1990s, when epidemiologist Maria Rosario Araneta joined UC San Diego’s faculty, she noticed a pattern: numerous patients at a nearby Veterans Administration hospital suffering from kidney damage due to diabetes were slim Filipino men. “They weren’t obese, they weren’t overweight,” Araneta says, emphasizing that “they had access to care” and were required to exercise as part of their Navy service.
This trend resonated with Araneta, a Filipina, because her father and grandmother both developed diabetes while appearing slim and healthy. “I thought – I’m definitely at risk. My community’s at risk,” she remembers.
Although there is a well-established connection between being overweight or obese and the risk of diabetes, Asians in America are 40% more likely to be diagnosed with the disease than whites, despite having lower average BMIs.
Dr. Alka Kanaya, a diabetes researcher and professor of medicine at UC San Francisco, suggests that one explanation could be that Asian bodies tend to store fat “in all the wrong places.” Instead of accumulating fat under the skin around the hips or thighs, Asian Americans often deposit it “in the liver, around the abdominal organs, in the muscle, around the heart.”
This can result in a condition known as “skinny fat,” where an individual may appear thin externally but possess a significant amount of visceral fat deep within the belly and surrounding the organs. Araneta explains that “visceral fat is not just a place where we store excess calories,” but rather, this hidden fat may contribute to Type 2 diabetes risk by promoting inflammation and insulin resistance.
Researchers are currently trying to determine how to reduce visceral fat, suspecting that building muscle might help, but they have yet to gather sufficient data to confirm this theory.
Adapting Screening Guidelines for Asian Americans
There is limited U.S. research funding available for studying diabetes in Asian populations, leading to issues with screening and underdiagnosis due to the historical lack of data. However, Dr. George King, founder and director of the Asian American Diabetes Initiative at the Joslin Diabetes Center in Boston, emphasizes that “it’s not that we have to wait for that for the research [to act]. There’s plenty we can do ourselves.”
King, Araneta, Kanaya, and other Asian American and Pacific Islander healthcare professionals successfully advocated for changes to screening guidelines. This was based on research indicating that many Asians develop diabetes at lower weights. In 2015, the American Diabetes Association began recommending that Asian Americans be screened for diabetes at a body mass index (BMI) of 23, instead of the BMI of 25 recommended for the general population.
The “Screen at 23” campaign helped spread this message, as Asian Pacific Islander physicians and others pushed for increased awareness and policy changes. Several states with high Asian populations have adopted these changes. The Asian American Diabetes Initiative provides a calculator that allows Asian Americans to check their BMI and determine if it falls within the at-risk or healthy range.
Double Screening for At-Risk Individuals
Araneta highlights issues with diagnostic tests, such as the A1C test, which measures blood sugar levels without fasting. An A1C level of 6.5% or higher indicates diabetes based on current medical guidelines, primarily derived from research on people of European descent. However, Araneta’s research shows that many Asians may have diabetes at lower A1C levels. In a study, the A1C test missed half of the Native Hawaiians diagnosed with Type 2 diabetes using the “gold standard” test and two-thirds of Japanese Americans.
This means that many Asians with diabetes might go undiagnosed for years until complications arise. To address this issue, Araneta and other researchers recommend that Asians with A1C levels in the “prediabetes” range (5.7% to 6.4%) undergo further testing for a more accurate diagnosis and proper interventions.
Understanding Subgroup Differences
Araneta stresses the importance of researching differences in diabetes risk among the diverse Asian American and Pacific Islander population, as some groups have much higher rates overall – South Asians, Filipinos, and Pacific Islanders. For example, while Chinese Americans generally develop diabetes at age 70 or older, South Asians tend to develop low insulin production at a younger age, leading to a subtype of Type 2 diabetes often associated with heart disease but not kidney problems, according to Kanaya.
Behavioural Changes for Prevention
While researchers continue seeking answers, doctors aim to reduce people’s risk now. The SAHELI diabetes prevention course that Shaheen Aamir participated in focuses on improving diet, exercise, and stress levels, proving even more effective than commonly prescribed drugs for warding off diabetes. The program is specifically adapted for South Asian foods and culture, addressing the stress of being an ethnic minority and the challenges faced when immigrating to a new environment.
Aamir credits the program with helping her change her family’s diet and lifestyle, resulting in weight management and increased energy to play with her children. Advocacy and prevention programs are making a difference, but the number of Asians and Pacific Islanders with diabetes continues to rise. Long-term lifestyle changes are needed to address the issue, and researchers are committed to this work for years to come.
The National Medical Commission (NMC) has approved 50 new medical colleges, resulting in the addition of 8,195 MBBS seats. The total count of MBBS seats in India now exceeds 1,07,658. However, concerns have been raised regarding the de-recognition of medical colleges due to non-compliance. According to official sources, 20 out of the 50 colleges who faced de-recognition threats have lodged appeals with the NMC. In addition, 102 medical colleges have received show cause notices for non-compliance, and six colleges have lodged an appeal with the health ministry. Some of these colleges are located in states including Maharashtra, Gujarat, Punjab, and others. “The medical seats in these colleges are reduced from that total count pending inquiry,” the sources added.
The 50 newly approved medical colleges are located in various states including Rajasthan, Maharashtra, Karnataka, Odisha, Tamil Nadu, Nagaland, Assam, Haryana, Gujarat, West Bengal, Uttar Pradesh, Jammu and Kashmir and Madhya Pradesh. The government considers this a significant increase in the number of medical colleges in the country since 2014.
The addition of new medical colleges will help in addressing the shortage of medical professionals in India. According to a report by the World Health Organization, India is short of 6,00,000 doctors and an equal number of nurses. With the approval of these new colleges, the Indian health system can take a progressive step towards addressing this shortfall. “This is an important achievement for the country, which has for long been struggling with a shortage of staff in the healthcare sector,” said a spokesperson.
The approval of 50 new medical colleges will significantly increase the number of MBBS seats available in the country. However, compliance issues remain a concern, and the authorities are taking action to ensure that medical colleges adhere to the required standards.
United Nations Secretary General Antnio Guterres on the eve of International Day of Yoga said that benefits of this ancient practice (Yoga) are precious in today’s dangerous and divided world.
“In a dangerous and divided world, the benefits of this ancient practice (Yoga) are particularly precious. Yoga offers a heaven of calm,” he said in a message on Tuesday, on the eve of the International Day of Yoga, which is observed on June 21 every year.
He further added that, “On this International Day of Yoga, let us embrace the spirit of unity, and resolve to build a better, more harmonious world for people, planet and ourselves.”
Prime minister Narendra Modi is set to lead a yoga session at UN headquarters in New York on Wednesday during the course of his ongoing US visit.
Following is UN Secretary-General António Guterres’ message for the International Day of Yoga, observed on 21 June:
The International Day of Yoga celebrates the restorative healing and inner peace provided by this ancient practice.
This year’s theme — Yoga for Humanity — reminds us how yoga is truly universal.
With roots in India, yoga is now practiced worldwide, giving people of all faiths and walks of life the tools and practices they need to enhance and balance their physical, spiritual and mental wellbeing.
For hundreds of millions of people worldwide, yoga has also been an essential lifeline during the COVID-19 pandemic, providing an important means of coping with the challenges of social isolation and stress.
And in a world beset by disaster and division, yoga’s values of mindfulness, balance, moderation and discipline are essential as we seek out a new relationship with one another and with our planet.
On this important day, let us be inspired by this timeless practice and its values.
INDIA New England News has announced that the 9th annual free Health, Fitness & Wellness Expo, New England’s premier health, fitness and wellness exhibition, will take place on August 13, 2023 at the Burlington Marriott Hotel in Burlington, MA.
The event will run from 10AM to 4PM, and feature exhibitors and speakers covering all aspects of health and wellness.
“We are excited to present our 9th annual in-person, immersive experience for all; and it is free for everyone to be healthy, fit and well,” said Upendra Mishra, publisher of INDIA New England News and the producer of the event.
For the last eight years, the Health, Fitness and Wellness Expo has organized expos featuring top panelists in their fields, including cardiology, internal medicine and medical entrepreneurship.
The expo is produced by The Mishra Group, in collaboration with INDIA New England News, Boston Life Sciences Times and IndUS Business Journal.
The expo was founded in 2013 by Mr. Mishra and Dr. Manju Sheth, MD, President of INE Multimedia.
The expo brings together the region’s top health and wellness providers, top speakers and fun workshops to promote life-long health, fitness and wellness in the Indian and South Asian community of New England. From free medical screenings to knowledgeable speakers to intensive yoga workshops, they bring the best options for a lifetime of health for the New England community.
The expo is free to attend for all registered participants. To register, please visit the link here on Eventbrite, or visit healthfitnesswellnessexpo.com.
INDIA New England News is New England’s oldest and largest print and online publication covering the Indian and South Asian community.
Updated daily, they cover the latest news in Bollywood, business, fashion, health, lifestyle, community events that touch the Indian and South Asian community.
Produced by the Mishra Group in collaboration with INDIA New England News, Boston Life Sciences Times and IndUS Business Journal, the Health, Fitness and Wellness Expo has organized expos featuring top panelists in their fields, including cardiology, internal medicine and medical entrepreneurship.
The expo brings together the region’s top health and wellness providers, top speakers and fun workshops to promote life-long health, fitness and wellness in the Indian and South Asian community of New England. From free medical screenings to knowledgeable speakers to intensive yoga workshops, they bring the best options for a lifetime of health for the New England community
The United States Food and Drug Administration (US FDA) has recently uncovered a series of regulatory failures in Indian pharmaceutical factories, raising concerns about the quality of drugs manufactured in the country. India is one of the largest producers of generic drugs, supplying approximately 40% of generic medicines consumed in the United States. Consequently, any lapses in manufacturing standards could have far-reaching implications for both the Indian pharmaceutical industry and patients relying on these medications.
The US FDA’s inspection reports reveal several instances of inadequate quality control measures, lack of data integrity, and improper sanitation practices in various Indian pharmaceutical plants. These issues have led to multiple warnings and import alerts from the regulatory body, which could potentially damage the reputation and export prospects of Indian drug manufacturers.
One such case involved Lupin Ltd., India’s third-largest drugmaker by sales, which received a warning letter from the FDA in November 2017. The warning cited significant violations of current good manufacturing practice (CGMP) regulations at two of the company’s facilities. Issues raised included insufficient oversight of suppliers, poor laboratory controls, and a lack of proper documentation.
Similarly, Dr. Reddy’s Laboratories, another major Indian pharmaceutical firm, faced an FDA warning in 2015 for CGMP violations at three of its manufacturing plants. The regulatory agency observed inadequate quality control systems, incomplete investigations into product failures, and a lack of data integrity in the company’s records.
These findings have prompted the Indian government to take action to improve the compliance of domestic pharmaceutical companies with international standards. The Central Drugs Standard Control Organization (CDSCO), India’s national regulatory body for pharmaceuticals and medical devices, has initiated efforts to strengthen its inspection processes and enhance collaboration with the US FDA.
To address the issue of data integrity, CDSCO is working on guidelines that will clarify expectations for Indian pharmaceutical companies regarding data management and record-keeping. The organization is also focusing on capacity-building initiatives, such as training programs for drug inspectors and regulatory staff to improve their understanding of CGMP requirements.
The Indian pharmaceutical industry has acknowledged the need to enhance its manufacturing standards and maintain transparency in its operations. Industry representatives have expressed their commitment to working closely with regulators to address these concerns and ensure the safety and efficacy of their products.
US FDA’s findings have highlighted significant shortcomings in the quality control measures employed by some Indian pharmaceutical factories. These revelations underscore the importance of stringent regulatory oversight and adherence to international manufacturing standards to safeguard public health. As the Indian pharmaceutical industry continues to expand its global presence, it must prioritize compliance with CGMP regulations and work collaboratively with regulatory bodies to uphold the highest standards of drug quality and safety.
Two US Congresswomen have introduced a bill to make it easier for the Department of Veteran Affairs to hire foreign employees on H1-B visas when they cannot find a suitable applicant in the country.
Introduced by Congresswomen Rashida Tlaib and Delia Ramirez on Thursday, the Expanding Health Care Providers for Veterans Act, will help address the healthcare provider shortage in the US by allowing immigrant health workers, who are H1-B visa holders, to offer the services that the veterans need.
The bill designates the Department of Veterans Affairs and State Veterans Homes as cap exempt institutions for the purposes of the H1-B visa program.
“We have a duty to uphold our commitment to our veterans, who are being affected by the health worker shortage in our nation. We can address this shortage with the immigrants in our communities who are ready and want to work, but face so many hurdles to do so,” said Congresswoman Ramirez, member of the House Committee on Veterans’ Affairs.
The Expanding Health Care Providers for Veterans Act was developed after the Detroit VA Medical Center nearly had to close their clinic — which provides life-saving care to more than 90 local veterans — earlier this year due to hiring difficulties imposed by the H1-B visa cap.
Representative Tlaib’s intervention was able to prevent the clinic’s closure, and this bill is designed to ensure such a situation does not arise again in the future, a statement released by the Congresswoman’s office said.
“Our veterans deserve high-quality health care, and our district knows firsthand the importance of providing access to care, especially mental health services for veterans who need it most,” said Congresswoman Tlaib.
“I am proud to introduce this legislation to expand healthcare providers for our veterans by welcoming healthcare professionals who are immigrants to care for them, and I will continue to ensure that our veterans are not forgotten when they return home,” she said.
This legislation is endorsed by The Veterans For Peace Save Our VA National Project and The American Immigration Lawyers Association. (IANS)
As we all know, May is National Nurses month and May 6 to 12 is National Nurses Week. On May 25, Dr Renee Mehrra of Reenbow Media and Indian American Forum organized a webinar in honor of National Nurses Week celebrations. Mrs. Indu Jaiswal, RDN and Chair of IAF together with Dr Urmilesh Arya Co-Chair of the event presented the program via ZOOM. Dr Renee Mehrra in her welcome remarks spoke about the importance of Health Care workers and to recognize for their services. Co Host of the evening Dr Bhavani Srinivasan spoke about the importance of Nurses in providing Quality care to patients all over the world.
Indu Jaiswal introduced Honorable Deputy Supervisor from Town of Hempstead MS Dorothy Goosby, who congratulated all Honourees and thanked Nurses and health care employees for their valuable services. Also present was Nassau County Legislature Rosemarie Walker, who thanked the nurses and congratulated all Honourees.
Tara Shajan, RN , NAINA Treasurer and Director of Nursing from Lincoln Hospital spoke about the history of Nursing profession, how Nurses are advancing in the Medical Field and paid tributes to Florence Nightingale, Lady with the Lamp.
Ms Anuradha Khanna started the program with Ganesh Vandana. Five nurses were recognized, and presented with Citations from Nassau County Executive Bruce Blakeman and Nassau County Legislature Rosemarie Walker
Suda Sharma: Born in Nairobi, studied in London and worked in USA as Registered Nurse. Along with Nursing, she is the founder of Three Community projects that started 19 years ago. She started the Annual Food Drive for Long Island Soup Kitchens and Homeless Shelters., Penny project for Foster Children, and Fundraiser for Safe Home. Suda is very active in all community activities.
Jaya Bahadkar studied Nursing in Bombay and has worked in Nursing in the USA for more than 25 years. She is also a Pillar of Indian American Community, very active in IALI, IAF, India Home and several other organizations’ is was recognized by Assembly woman Michele Solages Office Woman of Distinction Award in 2019.
Tara Shajan was born in Pondicherry, India graduated in Nursing. She has her private pilot license. In 2004 migrated to USA and worked as RN, progressing into leadership experience in Health care services, She is currently Treasurer for NAINA, Director of Nursing in Lincoln Hospital Tara is also very active in community services in USA and has received several awards.
Suja Madhu Studied Nursing in India and is a nurse for more than 40 years. Migrated in the USA in 1987 and started working as an assistant nurse manager in 1992 in Northwell. In 2008 transferred to Zucker Hillside Hospital and continues to work there still. She has been recognized as the Nurse of the Year award 2023for Northwell Health…
Grace Alexander was commissioned from Secunderabad as Lieutenant and midwifery from INHS ASVINI. After few years of work in Medical surgical floors, she worked at University Hospital in Saudi Arabia for 15 years and migrated to US in 2006. She has 20 years of experience as a med-surgical nurse and 15 years in OR. She is a Life member of NAINA and AORN. Currently she serves as Awards and scholarship chair in INANY 2021-2022 and member of scholarship committee.
Several distinguished members joined and praised the efforts of Nurses and their profession. Dr Rajiv Jauhar, Chief of Cardiology at North shore University hospital also commented on the importance of Nursing staff and their contributions in patient care in the Hospitals.
Dr Jagdish Gupta, a past President of the biggest County Medical Society in the State of New York and serving Brooklyn Community as a Physician for 50 years, said, “I truly believe that Nurses are an integral part of our healthcare team, and they play the most significant role in the care of our patients while in the hospital during the most critical period. Physicians, no doubt as leader of the team, are very important but, with time constraints, are only able to spend limited time. Servicing and caring are left to nurses, so much so, that it has become part of the fabric of their DNA to serve since Florence Nightingale time. Their compassion, dedication and expertise make a remarkable difference in the lives of countless patients every day. As a community leader and President of AIA(NY) Chapter, I am grateful for their unwavering commitment to providing exceptional care and making a positive impact on the World. During this “National Nurses Appreciation week. We honor and celebrate you as you are true heroes in every sense, today and every day.”
Gobind Munjal, National President of The Association of Indians in America (AIA) said, “May 6 is National Nurses Day, an annual opportunity to appreciate the nurses in our lives and remind ourselves of the innumerable ways they contribute to our health and the well-being of those we love. People have celebrated nurses for decades, but it wasn’t until the 1980s that the United States honored these integral healthcare professionals with their own day of recognition. National Nurses Day is the first day of National Nurses Week, which takes place from May 6-12 each year and concludes on International Nurses Day, the birthday of Florence Nightingale.”
The 2023 Nurses Week theme “Nurses Make a Difference: Anytime, anywhere – Always”
Nurses work every day to ensure patients get the care they need — and the comfort and compassion they deserve. The complex nature of nursing continues to be physically and emotionally draining, yet nurses carry on providing quality patient care and moving the profession forward, which reinforces the importance of nurse appreciation.
“Nurses need to be emotionally, psychologically, and morally refueled regularly to enable them to resist burnout and its many negative impacts such as moral distress,” said Bonnie Barnes, FAAN, Co-Founder of the DAISY Foundation, in a Nurse.com blog. One way to do this is through expressions of gratitude.“Nurses are refueled when they know they have made a difference in the life of a patient or family member, especially when they were unaware of the difference they made,” said Barnes.
This is why nurse appreciation events are so important. Nurses’ contributions are celebrated and recognized each year — as they should be — through special nurse appreciation days, weeks, and months set aside to honor nurses and their specialties.
Thanks to the Honorees and all nurses. We do appreciate the work that they do. Happy Nurses week to all the nurses present here. The webinar was well attended and some of the Community members present were Mrs. Neelam Modi, MS Nalini DAS RD, Sandy Bhatia, Dr Usha Bansal, Mr Amba Sharma, Dr Sollymol Kuruvilla RN PHD, Dr Shyla Roshin RN DNP,Mr Paul Panakal RN MSN, Dr Esther Devadas RN DNP the webinar was successful with the cooperation of Mrs. Flora Parekh Mrs. Beena Kothari, Anju Sharma, Sanju Sharma, Dr Renee Mehrra, Dr Bhavani Srinivasan and Dr Urmilesh Arya. For further details check Website www.indianamericanforum.org.
According to the latest Lancet Global Health Research Review on the Global Impact of Tobacco Control Policies on Smokeless Tobacco Use, India’s efforts to reduce smokeless tobacco consumption have been lauded as “exemplary.” The review highlights India’s comprehensive approach, which aligns with the WHO FCTC and encompasses various measures such as taxation, regulation, labeling, education campaigns, cessation services, and restrictions on sale to minors. The review specifically mentions the ban on smokeless tobacco products like gutkha, along with mandatory depiction of harmful ingredients and pictorial health warnings on packaging. These efforts are commended as exemplary by the review.
The Global Adult Tobacco Survey (GATS) 2 conducted in 2016-17 revealed that the overall prevalence of tobacco users in India was 28.6%, with smokeless tobacco users comprising 21.38% of the population. These numbers indicate a decrease compared to the earlier GATS 1 survey, which reported 34.6% overall tobacco users and 25.9% smokeless tobacco users.
Additionally, India has implemented various policies to discourage tobacco consumption and protect public health. These include bans on advertisements, the prohibition of plastic sachets for packaging, and restrictions on tobacco use in public places. Notably, some states in India, such as Maharashtra, Haryana, Uttar Pradesh, Bihar, Jharkhand, Uttarakhand, Telangana, Nagaland, and Assam, have issued orders to ban smokeless tobacco products and spitting in public places, particularly in response to the COVID-19 pandemic.
However, experts have highlighted the need for more stringent implementation of tobacco-related bans in India, as several states have been lax in enforcing them.
Globally, smokeless tobacco use affects approximately 300 million people, leading to significant contributions to tobacco-related diseases and deaths. Many countries have adopted policies beyond the WHO Framework Convention on Tobacco Control to address smokeless tobacco control, which has been effective in reducing smoking prevalence.
The use of smokeless tobacco products, including pan masala, gutkha, and khaini, is a significant public health concern in India and the Southeast Asian region. Earlier estimates indicated that nearly 80% of smokeless tobacco users reside in Southeast Asia, with around 60% in India.
On World Tobacco Day, Poonam Khetrapal Singh, the WHO regional director for South-East Asia, emphasized the success stories from countries like Bangladesh, India, Indonesia, and Sri Lanka, where tobacco-growing farmers have transitioned to economically viable alternative crops. Singh called upon all partners to support governments in tobacco-growing countries to develop and implement suitable policies and strategies for farmers to shift to growing food crops, leading to improved livelihoods, national economies, and food security.
The Lancet review, which marks the first systematic assessment of the global impact of tobacco control policies on smokeless tobacco use, involved a meticulous examination of 11 electronic databases and literature from January 1, 2005, to September 20, 2021. The findings revealed that 57 countries have implemented policies specifically targeting smokeless tobacco, with 17 of them going beyond the scope of the World Health Organisation (WHO) Framework Convention on Tobacco Control (FCTC).
The review highlights that policy initiatives based on the WHO FCTC have led to reductions in smokeless tobacco prevalence. For instance, taxation measures have resulted in reductions ranging from 4.4% to 30.3%, while multifaceted policies have yielded reductions ranging from 22.2% to 70.9%. The implementation of Article 11 (Pictorial health warnings) and Article 13 (Tobacco advertisement, promotion, and sponsorship ban) of the WHO FCTC has been widespread and impactful.
Experts have emphasized the need to scale up tobacco-related research in light of these findings. Ravi Mehrotra, co-author and member of the ICMR’s India Cancer Research Consortium, stressed the significance of increasing taxation and improving the implementation of existing laws. He stated, “Given that 300 million people use it worldwide, emphasis on increasing taxation and better implementation of the existing laws is of paramount importance. While policies on smokeless tobacco prevention and control exist in various countries, there is a lack of comprehensive research and assessment of their impacts, with limited publication in prominent tobacco reports or scientific literature.”
The review also emphasizes the importance of continuously updating guidelines and frameworks to incorporate new evidence on effective smokeless tobacco control measures. This reflects the need to stay abreast of emerging research and adapt strategies accordingly to enhance smokeless tobacco control efforts.
An increasing number of states are taking action against Big Tech, the internet, and social media platforms. Montana recently became the first state to entirely ban TikTok, though the enforceability of this new law remains questionable. Other states, such as Arkansas and Utah, have introduced legislation to tighten regulations on social media platforms.
There appear to be three primary objectives behind these legal actions: preventing companies from collecting data on users and their children, safeguarding children online, and striking a balance between users’ rights and responsibilities when posting content online. For instance, should a platform be held accountable if it hosts content that results in harm to someone? As of now, the US Supreme Court has ruled “no.”
As a father of three teenage girls, I find the conversations surrounding smartphones and social media deeply personal. Like many parents, I initially viewed devices as mere entertainment for my children and a means of communication in emergencies. However, my perspective changed after reading Jean Twenge’s book, “iGen: Why Today’s Super-Connected Kids Are Growing Up Less Rebellious, More Tolerant, Less Happy – and Completely Unprepared for Adulthood – and What That Means for the Rest of Us.”
In her book, Twenge, a psychology professor at San Diego State University, argues that Generation Z (or iGen) is experiencing a fundamentally different upbringing than previous generations. She informed me that some of the most significant behavioral changes in human history coincided with the advent of smartphones. According to Twenge, today’s 12th-graders resemble eighth-graders from earlier generations, delaying participation in activities associated with independence and adulthood. They are less likely to socialize, drive, attend prom, or consume alcohol compared to their Gen X counterparts, instead spending more time scrolling through social media feeds. Though they may be physically safer, the long-term impact on their mental and brain health remains uncertain.
Twenge shared with me that she “saw just a very, very sudden change, especially in mental health but also in optimism and expectations … between millennials and iGen or Gen Z.” Her words resonated with me but also alarmed me. As a neurosurgeon, I often rely on evidence to address concerns, but when it comes to new technologies, there is a scarcity of data available. We frequently don’t even know what questions to ask, let alone have answers for them.
Consequently, my wife, Rebecca, and I found ourselves in a challenging and uneasy position: determining the appropriate age, duration, and type of screen time for our three iGen daughters based on limited information. I know I’m not alone in this struggle, as I often hear similar concerns from other parents, viewers, readers, and listeners. This is why my podcast, “Chasing Life,” dedicated an entire season to discussing this topic.
Examining the Data
Obtaining consistent statistics is challenging, but a 2023 survey conducted by reviews.org revealed that approximately 89% of American adults check their phones within 10 minutes of waking up. Astoundingly, the same survey indicated that American adults look at their phones an average of 144 times per day, or once every seven waking minutes!
The numbers for children are even more concerning. A 2022 Pew survey of individuals under 18 years old showed that 46% of American teens reported being online “almost constantly.” Additionally, 35% claimed to be “almost constantly” using one of the top five social media apps: YouTube, TikTok, Instagram, Snapchat, and Facebook.
These statistics may not be surprising, considering the endless content available for consumption. In April 2022, data company Domo reported that over 500 hours of video were uploaded to YouTube every minute on average. Meanwhile, an estimated 1.3 billion photos are shared on Instagram daily, according to a photo industry estimate. Furthermore, Snap Inc. stated that over 4 billion Snaps were sent each day as of 2020.
My daughters, aged 17, 16, and 14, are digital natives who have never experienced life without devices. I often think about how this is not the world they chose, but rather the one we handed to them. My youngest daughter once expressed her wish to be a millennial because that generation had phones without smartphones or social media, so they weren’t constantly tethered to their devices. She says that many teenagers today feel compelled to use social media, fearing they will be left behind otherwise.
Lessons Learned
It’s undeniable that screens and technology play a crucial role in modern life, but managing our interactions with them can be challenging. While working on this season of the podcast, I gained valuable insights from experts in the field.
To summarize my findings, I would highlight three main points:
Initiate a meaningful conversation with your child, free from distractions and judgment. By discussing their screen usage, social media preferences, and feelings about online interactions, you may gain surprising insights and foster a more open dialogue. Dr. Michael Rich, co-director of the Clinic for Interactive Media and Internet Disorders at Boston Children’s Hospital, emphasizes the importance of understanding the pain points of young patients, saying, “I want to look more at what their life is from the time they wake up to the time they go to sleep.”
Avoid assuming the worst. While it’s likely that your child spends more time on screens than you’d prefer, not every individual will develop a problem. Dr. Keneisha Sinclair-McBride, a clinical psychologist at Boston Children’s Hospital and an assistant professor of psychology at Harvard Medical School, reminds us that social media isn’t the primary concern for most teens. She explains that the challenges faced by today’s youth are similar to those of previous generations, adding, “It’s not like every kid is going to get mental health treatment because social media is ruining their life. That is definitely not the case at all.”
Keep in mind the words of author Catherine Price: “Life is what we pay attention to.” This empowering concept reminds us that we have control over our experiences. When using our devices, Price suggests asking ourselves three questions: What for? Why now? What else? She explains, “The point is just to make sure that when we’re using our devices or whatever apps are on our devices, it’s the result of an intentional choice instead of just our minds and our brains being hijacked.”
By following these guidelines and making conscious choices, we can navigate the digital landscape more effectively and maintain a healthy balance in our lives.
Navigating the world of screens While exploring the topic of problematic media use during this podcast season, I’ve considered various metaphors to describe it. Is it an addiction like substances or gambling? Are devices designed to keep us hooked? While there are similarities, one key difference is that it’s not feasible to completely avoid technology.
A more fitting analogy might be food: we need both, but we must be mindful of our consumption. Another comparison could be a car or powerful tool: useful and impressive, but requiring control and proper handling. We should view these small supercomputers as tools, not toys for young children.
Did Rebecca and I flawlessly navigate this with our girls? No, but we didn’t have a precedent. “It didn’t exist when we were young, so we are learning how to manage it ourselves,” Rebecca stated. We’re adapting to the learning curve alongside our children.
The kids will be alright Technology is neither good nor bad; it just is. Gen Z acknowledges this and wants improvements. Advocates like Emma Lembke demand change, and lawmakers and tech executives are starting to listen. Lembke told Congress, “Make no mistake, unregulated social media is a weapon of mass destruction that continues to jeopardize the safety, privacy, and well-being of all American youth. It’s time to act.”
Lembke envisions a future where social media is built differently, with more transparent algorithms, an end to autoplay, and image filters that don’t perpetuate beauty standards. She and her peers are concerned for future generations.
We must learn to make better decisions about our digital diets. Dr. Keneisha Sinclair-McBride reminds us that our time and attention are valuable resources, and we should allocate them wisely.
Starting the screentime conversation Unsure how to discuss internet and social media use with your kids? Here are some conversation prompts:
Describe your typical phone usage in a day.
How much time do you spend on your phone daily? Too much, too little, or just right?
What are your favorite apps, games, or platforms, and why?
Do you have a healthy relationship with technology and social media? What does that look like?
Do you have fair screentime boundaries? Are they easy to stick to? Would you change the rules?
Has technology ever interfered with an activity you wanted to do?
Do you feel pressure from friends or school to be on your phone?
Do you know people who misuse technology?
What concerns you about technology or social media?
Have you tried reducing screentime? Why, and did it work?
(Philadelphia, PA: May 26, 2023) “The 41st Annual AAPI Convention & Scientific Assembly scheduled to be held from July 6th to 9th, 2023 will feature world-renowned leaders in healthcare and academia, who are well known and are sought after around the world for their expertise and knowledge,” said Dr. Ravi Kolli, President of The American Association of Physicians of Indian Origin (AAPI). “The multidisciplinary Continuing Medical Education (CME) during the convention allows specialists and primary care physicians to interact in an academic forum. The speakers at the CME will lead discussions on gaps between the current and best practices on wide-ranging topics,” he added.
It’s a well-known fact that physicians of Indian origin excel in their respective areas of work and continue to play key roles in patient care, administration, academics, and medical research. In order to cater to its diversity of medical specialties, AAPI continues to use a multi-disciplinary conference format. “The essence of AAPI is educational,” said Dr. Ravi Kolli, while describing the purpose of CME said.
“The 41st annual AAPI Convention in Philadelphia will provide physicians of Indian origin an opportunity to come together in an atmosphere of collegiality, enabling them to retrace and appreciate their common roots, culture, and bond that unites them as members of this large professional community,” said Dr. V. Ranga, Chair of AAPI BOT.
Picture : TheUNN
According to Dr. Anjana Samadder, President-Elect of AAPI, “This mission of AAPI translates into numerous CME and non-CME seminars by experts in their fields. CME will provide comprehensive and current reviews and guidelines for the diagnosis and treatment of various disease states to reduce morbidity and mortality and achieve cost-effective quality care outcomes. At the end of the activity, it is expected that attendees will gain an understanding of the causation, diagnosis, and best clinical practices for the management of the diverse group of diseases discussed during this program.”
Led by Dr. Sreeni Gangasani, AAPI CME Chair and Dr. Brahma Sharma, AAPI Convention CME Chair, the CME Committee has Drs. Gunjan Shukla, Sunder Rao, and SACHIN MEHTA as members.
“As the Chair of the AAPI CME Committee, I am proud to announce that our program will be providing the highest level talks for AAPI delegates,” said Dr. Sreeni Gangasani. “Our team has worked tirelessly to curate a lineup of speakers and presentations that will provide valuable insights and information to our attendees. We understand the importance of staying up-to-date on the latest research, trends, and best practices in healthcare and beyond, which is why we have chosen speakers who are experts in their fields and who are passionate about sharing their knowledge with our delegates. We hope that our program will inspire and empower our attendees to make a positive impact in their communities and beyond.”
According to Dr. Brahma Sharma, Chair of AAPI Convention CME Chair, “CME has been a major highlight of AAPI conventions. This year, our teams’ approach has been holistic and balanced, with sessions focusing on both old and new: bedside and bench side and usual care, in addition to personalized approach to chronic diseases which have become our nemesis today. The goal is not just to educate about current concepts of chronic disease management but also inform about emerging concepts like Genomics, Gene-editing, and Artificial Intelligence, which play a critical role in managing chronic conditions. AAPI has been fortunate to be able to tap in some of the world’s leading physician-scientists in these areas of Medicine.”
In addition, there is the popular parallel track for Life style Medicine, which touches Mind- Body side, making it a wholesome CME session, giving everyone something that they would love. I thank Dr. Ravi Kolli for giving me the opportunity to work with him and his team during the convention. I hope all these will be informative as well as enlightening CME sessions, Dr. Sharma added.
The inaugural CME session on July 6th is being led by Dr. Satheesh Kathula, Clinical Professor of Medicine and a Board Certified Hematologist and Oncologist, who will address the delegates on “Rise of Immunotherapy in Lung Cancer.” Dr. Sujeeth R Punnam, an Interventional, Structural Cardiologist & Certified Cardiac Device Specialist in Stockton, CA will present on: “Update and Long term outcomes on Transcatheter Aortic Valve Replacements.”
Dr. Prasad Chalasani, an Interventional Cardiologist at the Florida Heart Center and the Chief of Cardiology at Lawnwood Regional Medical Center & Heart Institute; Clinical Associate Professor at Florida State University School of Medicine and at Florida Atlantic University School of Medicine will share insights on “Role of LAA Left Atrial Appendage Closure in Atrial Fibrillation.”
“Advancing Access to Care through Licensure Portability and Telemedicine” will be the topic addressed by Dr. Humayun Chaudhary, President and CEO of FSMB. Dr. Vikas Khurana, Program Director of the Gastroenterology Fellowship Program at The Wright Center for Graduate Medical Education will share his expertise on: “Inflammatory Bowel Disease in South Asian Patients.”
Chronic Disease: Non-Communicable Diseases is the theme for the CME session on July 7th. Dr. Pradeep Natarajan, Director, Preventive Cardiology MGH, Associate Professor Harvard Medical School will lead the day’s sessions by focusing his address on: “Subclinical Atherosclerosis in South Asians: Early Detection and Management.” This will be followed by a session led by Dr. Sunder Rao, Senior Consultant at the Butler Health System MARS PA on: “Role of SGLT2 in Preventing Heart Failure.”
“Contemporary Approach in Prevention and Management of CKD” is the theme addressed by Dr. Wilcox Christopher, Chief Division of Nephrology and Hypertension, Georgetown. Dr. Rajnish Mago, Clinical Assistant Professor at the
University of Pennsylvania will speak about: “Current Concepts in Management of Bipolar Depression.”
Dr. Surender Neravetla, Cardiothoracic Surgeon, Ohio will provide education on: “Role of Diet/Salt in Pathogenesis of Chronic Disease.” Dr. Indranill Basu Ray, MD
Founder President of the American Academy of Yoga in Medicine will share his insights on: “Yoga/Meditation in Chronic Disease Management.”
Dr. Indira Gurubhagavatula, Associate Professor Medicine and Director Sleep Medicine at UPenn will speak about: “Sleep and Public Health Policy,” while the concluding session for the day will be led by Dr. Vemuri S. Murthy, Adjunct Faculty
at the Department of Emergency Medicine, University of Illinois College of Medicine
Chicago, Illinois, who will address the delegates on: “Update on Sudden Cardiac Arrests during COVID-19 Pandemic & Cardiac Arrest Registries, with Focus on India.”
The final day of the convention, July 9th will have “Frontier of Medicine” as the main theme. Dr. Sek Kathieresan, Director of Preventive Cardiology MGH, and Associate Professor, Harvard Medical School will lead an insightful session on: “Genomics and Gene Editing in Cardiovascular Disease.” Dr. Partho Sengupta, Professor CV Medicine at the Robertwood Johnson Medical School Rutgers University will share with the delegates on: “AI and Cardiovascular Imaging.”
“Percutaneous Mechanical Support in High-Risk PCI/ Cardiogenic Shock” is the theme addressed by Dr. Jon George, Director of Complex PCI at UPenn Hospital. Dr. BK Kishore, Academician, Innovator, and Entrepreneur, University of Utah Health and ePurines, Inc., Salt Lake City, Utah will lead the session on: “Impact of AI on Molecular Diagnosis and Therapy.”
Lifestyle Medicine Track will be the theme during the concurrent session on July 9th morning. Dr. Nina Vasan at the Department of Psychiatry, Stanford University will inaugurate the Track with her address on: “Mental Health and Social Media.” Dr. Natrajan Rangnathan, Founder and Lead Scientist will share his insights on: “Gut Biome/Dysbiosis and Chronic inflammation.”
“Personalized Diabetes Care and Glucose Device Monitoring” is the topic addressed by Dr. Bantwal Baliga, Chief Endocrinology Clinics, Georgia, and the concluding session will be led by Dr. Nori Dattatreyudu, Chair Oncology, NY Presbyterian Hospital, and will focus on: “Prevention and Precision in Cancer.”
“Giving them a platform to celebrate their accomplishments, the annual convention to be attended by nearly 1,500 physicians of Indian origin, it will also provide a forum to renew their professional commitment through continuing medical educations activities,” said Dr. Sanjay Gupta, Convenor of AAPI Convention.
“Physician leaders who will be part this convention have excelled in different specialties and subspecialties and occupy high positions as faculty members of medical schools, heads of departments, and executives of hospital staff. The AAPI Convention offers an opportunity to meet directly with these physicians who are leaders in their fields and play an integral part in the decision-making process regarding new products and services,” Dr. Raghu Lolabhattu, CEO of the Convention said.
American Association of Physicians of Indian Origin (AAPI) represents more than 100,000 Indian American Physicians and reflects the range of physician specialties seen in the physician community at large with 61% in Primary Care, 33% in Medical sub-specialties and 6% in surgical sub-specialties. Medical specialty representation includes pediatrics, psychiatry, anesthesiology/pain management, cardiology, family medicine, obstetrics and gynecology, oncology, gastroenterology pathology, endocrinology, nephrology, rheumatology along with many other fields.
AAPI is an umbrella organization that has nearly 250 local chapters, specialty societies and alumni organizations. For over 40 years, Indian physicians have made significant contributions to health care in this country, not only practicing in inner cities, rural areas and peripheral communities but also at the top medical schools and other academic centers. Almost 12% of medical students entering US schools are of Indian origin. Headquartered in Oak Brook, Illinois, AAPI represents the interests of over 100,000 physicians, medical students, and residents of Indian heritage in the United States. It is the largest ethnic medical organization in the nation. For more details and registration for the convention, please visit: www.aapiconvention.org and www.aapiusa.org
(Chicago, IL; May 26, 2023) India, home to one of the oldest medicinal systems in the world has made remarkable changes in medical education in the recent past. As the world is changing to meet the ever-changing needs, medical education in India is moving forward with the objective of rendering every medical graduate and postgraduate the best in the world. Several changes are being made for graduates from Indian schools to be at par and for easy mobilization around the world.
India is introducing the NEXT examination, which is the licensing examination similar to USML in the US, while the UKMLE is starting in the UK in 2024 in the place of PLAB examination.
NMC applied for WFME Recognition status, which is mandatory to apply for USMLE examination. 694 Medical schools in India with106,083 MBBs admissions a year selected from 2.1 million applicants through the UG NEET examination, one day across India in 3 hours. With the government policy of one medical college for every district to meet the Indian need,
medical education has many challenges in the transfer of knowledge and quality.
NBEMS is responsible for NEET PG Entrance Test, which is taken up by more than 200,000 students once a year. India’s Health Minister Mandaviya has said that the government of India is working to equal the number of medical UG and PG seats in 4 years: Post-graduate seats have grown from 34,000 to 64,000 in the last 8 years, the Union Health Minister said in a conference. To overcome the shortage of teachers in medical colleges, the Medical Council of India (MCI) has increased the professor-student ratio from 1:2 to 1:3 for postgraduate (PG) courses in all Medical Colleges from the 2018-19 academic session.
In this context, the American Association of Physicians of Indian Origin (AAPI) has led efforts to help streamline medical education in India to meet the global standards for medical practice around the world.
AAPI took the lead last month to bring together the leaders of National Board of Examination in Medical Science (NBEMS) India, National Board of Examination in Medical Science (NBME) USA, and the Federation of State Medical Boards (FSMB) on April 27th at the NBME office in the nation’s capital, Washington, DC.
Dr. Lokesh Edara, BOT-Chair Elect, and Dr. Sumul N. Raval, current Treasurer of AAPI and Secretary-Elect represented AAPI at the meeting.
NBME was represented by Dr. Peter Katsufrakis; Dr. Mike Jodoin, USMLE Program; Dr. Daniel Jurich, Growth and Innovation, Overview National Board of Examinations; and, Pamela Treves, Senior Vice President of NBME’s Growth and Innovation Division.
Dr. Abhijat Sheth represented NMBE – India. FSMB was represented by Dr. Humayun Chaudhry, President and CEO of the Federation of State Medical Boards.
“Overview National Board of Examinations” was the main theme discussed during the meeting. According to Dr. Lokesh Edara, Chair-Elect of AAPI Board of Trustees, “AAPI hoped the excellence gained through long term vision, insight and hard work with both organizations and exchange of ideas and challenges will benefit the medical education system in India and help tens of thousands of medical graduates coming from India to have recognition in the US.”
He urged Dr. Sheth to increase family medicine PG seats and nationalized formative assessment tests in theory part for all post graduates and for post-graduate exit theory examination suggested computerized online test. Nationwide E-Learning systems for higher transfer of Knowledge in medical education
Dr. Raval said, “In order for us to meet the unprecedented demand and to bring up the quality of education, the Indian medical education system is changing rapidly. The meeting today was a great beginning to facilitate collaborative efforts between India and the United States.”
Dr. Sheth presented the NBEMS mission and PG NEET examination, FMGE examination and more than 50 specialties for postgraduate and super specialties courses they are conducting and graduating. He invited all the participants at the meeting to their office in New Delhi during their next visit to India. AAPI leaders invited the leadership of these regulatory groups to the AAPI annual convention in Philadelphia in July 2023 and to the AAPI Global Healthcare Summit meeting in New Delhi in January 2024.
Dr. Katsufrakis provided an update on the NBME history and current examination-system. Dr. Katsufrakis is a board-certified Family Physician, whose professional focus has been to improve the quality of care provided to patients through effective assessment of health care professionals, and is leading the NBME to grow as an ally in helping health professionals maximize their mastery and performance.
Dr. Humayun Chaudhry, President and CEO of the Federation of State Medical Boards (FSMB), which was founded in 1912 and represents all 70 of the nation’s state and territorial medical licensing boards, represented FSMB at the meeting. FSMB operates the Federation Credentials Verification Service and co-manages the United States Medical Licensing Examination (USMLE) with the National Board of Medical Examiners.
Michael Jodoin is the Senior Vice President for Customer and Portfolio Management at NBME. In this role, he is accountable for the strategic and operational leadership for NBME’s portfolio of products and services and the customers and stakeholders that we serve.
Daniel Jurich serves as associate vice president for the USMLE® program. In this role, he leads and supports various validity, equity, and security initiatives that enhance the quality of USMLE for students, medical educators, clinicians, and licensing authority members.
Pamela Treves is the Senior Vice President of NBME’s Growth and Innovation Division. This division supports the organization’s strategic goals and vision by providing leadership to accelerate the pace of change and innovation for our products and services – in collaboration with medical education and health care to better support learners, advance assessment, and improve the care that patients receive.
Dr. Abhijat Sheth, President, National Board of Examinations, since 2016 completed his post-graduation in Cardiothoracic Surgery from Sheth KM School of Postgraduate Medicine and Research, Ahmedabad. He extensively worked as an academician at various medical colleges in India. He worked in SMT NHL Medical College while in UK , worked in four NHS Trust Hospitals, and as the Director of Medical Services at Apollo Hospitals International LTD, Ahmedabad in India.
Dr. Lokesh Edara, board certified in Allergy and immunology in Private practice since 1990, is a former President of the Michigan Allergy Asthma Society and former President of Calhoun County Medical Society. He serves as the President of the Association of Allergists and Immunologists from India 2001-2003. He is the Chairmen of AAPI Global Medical Education and Chairmen-Elect of AAPI Board of Trustees 2023-2024.
A board-certified neurologist and authority on brain tumors, Dr. Sumul N. Raval is one of the few neuro-oncologists in private practice in the United States. Dr. Raval is the founder and director of the David S. Zocchi Brain Tumor Center at Monmouth Medical Center – New Jersey’s first and most comprehensive facility specializing in brain tumors. He was recently elected as the Secretary of AAPI for the year, 2023-2024.
Expressing appreciation for Dr. Edara and Dr. Raval for taking the lead in facilitating interaction and dialogue between the Medical Education Boards of India and the United States, Dr. Ravi Kolli, President of AAPI said, “Since its inception over four decades ago, AAPI has been in the forefront advocating for medical school education reform and for the medical graduates from India to be treated on par with their counterparts in India. India is already leading the global pharmaceutical industry, and rebooting medical education will help India enter the league of leaders in healthcare around the world. The meeting today was a great start, and I look forward to AAPI continuing to lead such efforts in the coming years benefitting the medical fraternity.” For more information on AAPI and its many initiatives, please visit: www.aapiusa.org
Instead of relying on sugar substitutes, individuals should reduce their consumption of sugar-sweetened beverages and opt for raw or lightly processed fruit as a source of sweetness. The new guidelines aim to assist government health organizations in implementing policy changes based on the latest scientific analysis.
The World Health Organization (WHO) recommendation includes both low or no-calorie synthetic sweeteners and natural extracts, such as acesulfame K, aspartame, advantame, cyclamates, neotame, saccharin, sucralose, stevia and stevia derivatives, and monk fruit. According to Francesco Branca, stevia and monk fruit are newer sweeteners with less published research, but they likely share a similar physiological mechanism with other sweeteners. He states, “We cannot say they are different from the others based on the data we have — they play the same role.”
Branca emphasizes the importance of reducing dependence on free sugars and non-nutritive sweeteners, particularly in early childhood. Registered dietitian Lisa Drayer suggests training your taste buds by gradually cutting back on sugar, including artificial sweeteners, and incorporating more protein and fiber-rich foods into your diet. Additionally, she advises Sportschoosing no-sugar-added foods, avoiding sugar-sweetened drinks, enjoying fruit for dessert, and being aware of hidden sugars in various food products.
By checking nutrition facts labels and recognizing alternative names for added sugars, individuals can make healthier choices and reduce their sugar intake. This approach can help tame one’s sweet tooth and lessen dependence on sugar and sweeteners.
Dr. Sampat Shivangi, a physician, an influential Indian American community leader, and a veteran leader of the American Association of Physicians of Indian Origin (AAPI) was awarded the prestigious Lifetime Achievement Award by the Xavier University School of Medicine on Friday, May 19th, 2023 at the Xavier’s Campus in Aruba. Dr. Shivangi was conferred with the Life Time Achievement Award by the Honorale Minister of Aruba, Mr. Croes along with the President of Xavier University of School of Medicine Mr. Ravi Bhopalapu.
The award ceremony was part of the Global Leadership Summit organized by the University, which brought together world leaders in the Global Health Care community, who shared their insightful thoughts and expertise on various topics related to healthcare. The summit featured speakers from diverse backgrounds with areas of expertise, including healthcare policy, healthcare technology delivery, and healthcare education.
The summit was aimed at providing education not only to Xavier University School of Medicine students and faculty but also to healthcare professionals and educators, who are passionate about making a positive impact on the healthcare industry and improving patient outcomes worldwide.
“We are excited to bring together stingrays naked ladies from around the world did experiences and insights,” said Dr. Ravi Bhoopalpur, President of Xavier University School of Medicine. “The goal is to create a platform for the exchange of ideas and best practices that will help shape the future of healthcare and improve the lives of people around the world.”
In his response to being chosen for the award, Dr. Shivangi said, “I am truly honored to receive this prestigious Xavier University of Aruba award, which has made a worldwide impression as a premier Institute of learning. It’s even a greater honor to be in such distinguished ranks of those present and past honorees, who have made important contributions to healthcare.”
Describing the honor as “a significant milestone in my life and a moment to cherish,” Dr. Shivangi said, “Health care across the world is regarded as an important determinant in promoting the general, physical, mental, and social well-being of people around the world and can contribute to a significant part of a country’s economy, development, and industrialization when efficiently improving human health and providing access to affordable high-quality health care.”
Addressing the epidemic of mental health, Dr. Shivangi, a champion of women’s health and mental health, and whose work has been recognized nationwide, said, “Mental health illness continues to impact more people each year and is now a global disease.” Quoting the World Health Organization, Dr. Shivangi, said, “WHO estimates 1 in every 8 individuals worldwide suffer from a mental disorder, impairment in childhood, depression, anxiety, substance abuse, & psychosis in maturity and ending with dementia in old age. 5.6 crore Indians suffer from depression, while 3.8 crore suffers from anxiety disorders.”
Focusing on Mental Health, Dr. Shivangi said, “Mental Health literacy is the gateway for mental health intervention. However, there is a lack of awareness, which can lead to overlooking, misjudging or dismissing the signs that someone needs help. Dr. Sivangi, an obstetrician/gynecologist, the first Indian to be on the American Medical Association, the apex law-making body, pointed out that substance abuse in the United States causes over 10,000 youth to die annually.
Quoting studies that point to the fact that Mental Health has emerged as an “ever-challenging task,” Dr. Shivangi said, nearly 1 in 5 Americans has some type of Mental illness. During the Covid pandemic period, 78% of adults were experiencing a mental illness, an equivalent of over 50 million Americans, with millions of adults in the USA experiencing serious thoughts of suicide, with the highest rate amongst multi-racial individuals.
Responding to realities, the US Government has initiated several measures to help people struggling with mental health issues and substance abuse. In this context, he referred to two recent initiatives by the US Government to address the twin issues of mental health and substance abuse:
The exclusive 988 National Emergency Phone Number for the mentally ill has revolutionized the mental system that has saved thousands of lives and reduced by a third of hospital visits. In addition, making the antidote, Naloxone free of cost and available over the counter has helped save so many lives.
Dr. Shivangi said, one can get instant help by calling #911 in crisis; they can call or Text #988 Suicide & Crisis Lifeline, a new Nationwide service, attended by trained staff, and trained crisis counselors who can counsel, guide and get them admitted into nearby crisis center, community mental health center or hospital immediately that includes ambulance service. “This has caught nationwide attention. I would strongly recommend that Aruba should think along these lines.”
The SAMHSA Substance Abuse and Mental Health Services Administration is another major initiative of the US government. Dr. Shivangi serves on the Board of SAMHSA, a prestigious position, appointed by the President of the United States. I was first appointed by President Trump & now by the current President Joe Biden.”
Recalling his recent visit to Poland, where Dr. Shivangi shared about the huge impact through these initiatives, Dr. Shivangi said, the government of Poland was impressed and wanted to use them in their country as a way to save lives. Dr. Shivangi offered similar programs and services made available to the people of Aruba and was open to helping the Government of Aruba make them part of the healthcare delivery in the island nation.
A conservative lifelong member of the Republican Party, Dr. Shivangi is the founding member of the Republican Indian Council and the Republican Indian National Council. Dr. Shivangi is the National President of Indian American Forum for Political Education, one of the oldest Indian American Associations. Over the past three decades, he has lobbied for several Bills in the US Congress on behalf of India through his enormous contacts with US Senators and Congressmen.
A close friend to the Bush family, he was instrumental in lobbying for the first Diwali celebration in the White House and for President George W. Bush to make his trip to India. He had accompanied President Bill Clinton during his historic visit to India. Dr. Shivangi is Dr. Shivangi has worked enthusiastically in promoting India Civil Nuclear Treaty and recently the US India Defense Treaty that was passed in US Congress and signed by President Obama.
Dr. Shivangi has actively involved in several philanthropic activities, serving with Blind foundation of MS, Diabetic, Cancer and Heart Associations of America. Dr. Shivangi has number of philanthropic work in India including Primary & middle schools, Cultural Center, IMA Centers that he opened and helped to obtains the first ever US Congressional grant to AAPI to study Diabetes Mellitus amongst Indian Americans.
Dr. Sampat Shivangi was awarded the highest civilian honor, the Pravasi Bharatiya Diwas Sanman award in 2016 in Bengaluru by the Hon. President of India, Shri Pranap Mukhejee. He was awarded the prestigious Ellis Island Medal of Honor in New York in 2008. He is married to Dr. Udaya S. Shivangi, MD, and the couple are blessed with two daughters: Priya S. Shivangi, MS (NYU); Pooja S. Shivangi who is an Attorney at Law.
A staggering 70% of US adults believe the health care system fails to address their needs in at least one aspect, as revealed by recent data from the Harris Poll, obtained exclusively by TIME.
Although the US spends more per capita on health care than any other affluent nation, it lags behind in terms of life expectancy and various health outcomes. The Harris Poll survey, carried out between February and March 2023 and commissioned by the American Academy of Physician Associates, indicates that patient satisfaction is also being negatively impacted by the exorbitant costs, lack of accessibility, and convoluted logistics associated with US medical care.
When questioned about their personal grievances with the medical system, many respondents cited similar issues. A mere 27% of those surveyed claimed the US medical system fulfilled all their needs, while the remaining participants voiced concerns regarding appointment wait times (31% of respondents), high costs (26%), insurance coverage limitations (23%), and inadequate emphasis on preventive care and wellness (19%).More than a fifth of people surveyed said they don’t see a single health care provider on a regular basis, and 44% said they’d skipped or delayed needed care in the past two years.
Despite these challenges, the survey also highlighted potential areas for improvement and progress. Over 75% of respondents acknowledged that providers collaborate with them to enhance their health, while more than 70% expressed a desire for stronger relationships with their providers. Furthermore, over 65% believed their health would improve if they consistently worked with a trusted provider. These responses imply that Americans haven’t entirely lost faith in the system, even in the face of their frustrations.
Federal health advisors announced on Wednesday that a long-standing birth control pill could potentially be sold over the counter, potentially leading to the first non-prescription contraceptive medication in the U.S. A panel of FDA advisors unanimously supported Perrigo’s proposal to sell its daily medication alongside products like eye drops and allergy pills. The recommendation came after a two-day meeting discussing whether women could safely and effectively use the pill without professional supervision. The FDA is expected to make its final decision this summer.
Picture : WTSP
If the agency follows the non-binding recommendation, Perrigo’s drug, Opill, would become the first contraceptive pill available without a prescription. The company stated that sales could commence late this year if approved. External experts mostly expressed confidence that women of all ages could use the drug appropriately without consulting a healthcare provider first.
“In the balance between benefit and risk, we’d have a hard time justifying not taking this action,” said Maria Coyle, an Ohio State University pharmacist who chaired the panel. “The drug is incredibly effective, and I think it will be effective in the over-the-counter realm just as it is in the prescription realm.”
Despite numerous criticisms from FDA scientists regarding how Perrigo studied the drug, including questions about whether study participants could understand and follow labeling instructions, the panel largely dismissed these concerns. Instead, they emphasized the advantages of providing more effective birth control, particularly to young people and lower-income groups, than what is currently available over the counter, such as condoms and gels.
Opill belongs to an older class of contraceptives containing only progestin, which generally has fewer side effects and health risks but may be less effective if not taken consistently at the same time daily. Although the FDA’s decision will not apply to other birth control pills, advocates hope that an approval might encourage other drugmakers to seek over-the-counter sales. In many parts of South America, Asia, and Africa, birth control pills are available without a prescription.
Approved in the U.S. five decades ago, Opill was shown to be over 90% effective in preventing pregnancy when taken daily. However, it remains uncertain how popular it might be if approved for over-the-counter use, as Opill has not been marketed in the U.S. since 2005.
Certain women, particularly those with breast cancer, should avoid taking Opill due to the risk of accelerating tumor growth. Women experiencing unusual vaginal bleeding are advised to consult a doctor before using it, as bleeding could signify a severe health issue. However, in reading comprehension studies conducted by Perrigo, 68% of women with unexplained bleeding incorrectly believed they could take the drug. A few women with breast cancer also indicated they could use Opill.
Panel members noted that nearly all women with a history of breast cancer would be under the care of a cancer specialist who would advise against taking hormonal drugs that could exacerbate their condition. “I would think any woman who had a breast cancer diagnosis in the past would be highly aware of that, so I don’t think that’s going to be a concern,” said Dr. Deborah Armstrong of Johns Hopkins University.
Perrigo claimed its 880-patient study demonstrated that women would consistently take the pill daily if made available over the counter. However, the FDA identified several issues with the study, including over 30% of participants who mistakenly reported taking more pills than they were given. FDA reviewers argued that this problem cast doubt on the company’s overall conclusions about the drug’s use and effectiveness.
FDA regulators also suggested that changes in U.S. demographics since the pill was first tested—including increased obesity and other chronic conditions—could diminish the drug’s effectiveness. Despite these concerns, Opill has garnered support from numerous reproductive rights and medical groups advocating for broader access to birth control.
“Opill over the counter would give us one more option for access and the more options that are available the better,” stated Clare Coleman, president of the National Family Planning and Reproductive Health Association. Coleman was among over 25 speakers who endorsed Perrigo’s application during a public comment session on Tuesday.
Catholic organizations, including the United States Conference of Catholic Bishops, oppose the move, arguing that women should be evaluated by a doctor before receiving the drug. Perrigo has not publicly discussed pricing for the drug if approved. Non-prescription medications are typically less expensive, but they are generally not covered by insurance. Requiring insurers to cover over-the-counter birth control would necessitate a regulatory change by the federal government.
After more than three long years, the Covid-19 pandemic is finally coming to an end. On Friday, the World Health Organization (WHO) announced that Covid-19 no longer poses a Public Health Emergency of International Concern, while the United States is set to end its own public health emergency declaration on Thursday. However, this news doesn’t mean that the world is entirely out of the woods. “Although it is a very good sign, it doesn’t mean America or the world is entirely out of the woods,” states a recent news article.
Throughout the pandemic, the United States has been described as a patient by numerous health experts. The end of the public health emergency can be considered as the patient’s discharge from the hospital after a lengthy illness. This discharge follows numerous setbacks and improvements, from stints in the ICU to triumphs of modern medicine and human ingenuity.
However, it’s imperative that all countries keep a close eye on the situation as Covid-19 is still a global threat. Last week, the WHO’s International Health Regulations Emergency Committee decided that the Public Health Emergency of International Concern (PHEIC) should end as a result of decreasing Covid-19-related hospitalizations and deaths, as well as high levels of immunity in the population. The committee advised that it’s time to transition to long-term management of the COVID-19 pandemic.
“During the process of transitioning from emergency to long-term, the level of concern is lower,” said Maria Van Kerkhove, WHO’s Covid-19 technical lead and head of its program on emerging diseases. “While we’re not in crisis mode, we can’t let our guard down. The disease and the coronavirus that causes it are here to stay.”
The WHO also wants to ensure that the pandemic is under control and that everyone follows health regulations, including testing, monitoring, and follow-up appointments, to prevent the possibility of a readmission.
“Covid-19 is still a global threat because the virus can continue to evolve and spread,” said Van Kerkhove. “We need to carefully watch for new variant strains, especially in unvaccinated populations. We also need to ensure that vaccines are accessible to everyone, regardless of where they live.”
The United States has designated May 11 as the date to end its public health emergency, which was declared in response to the pandemic caused by the SARS-CoV-2 virus. The declaration, which has been renewed 13 times, has given the US government wide-ranging flexibility in the fight against COVID-19. It has allowed for the implementation of certain policies and actions, such as a wider social safety net and free access for Americans to COVID-19 vaccines, tests, and treatments. However, as the pandemic situation improves, the US Centers for Disease Control and Prevention (CDC) will lose access to some data used to measure the severity of the pandemic and guide its public health recommendations.
Dr. Rochelle Walensky, CDC Director, said that at the end of the public health emergency, the CDC will have less access to data. “We will lose our percent positivity. We won’t get laboratory reporting. We won’t get case reporting. So we’ll lose some of that,” she said. Nevertheless, the CDC is “not changing the steam at which we are working through this resolving this public health emergency.” The agency will continue to closely monitor the virus around the country, using novel approaches like genomic sequencing and wastewater testing.
The expiration of the public health emergency declaration means an end to some programs and actions, while others will wind down slowly, and some will remain in place. The US Department of Health and Human Services announced the extension of the public health emergency for the last time, subsequently allowing it to expire. The decision means that the government will no longer have the wide-ranging flexibility it once had in the fight against the pandemic.
Despite the end of the public health emergency, many Americans remain concerned about the pandemic. Experts say people must remain vigilant in adhering to precautions, such as wearing masks and social distancing, to prevent a resurgence of COVID-19 infections. The CDC recommends that people continue to get vaccinated and follow its guidelines for preventing the spread of the virus.
The end of the US public health emergency does not mean the end of the pandemic. It marks a significant milestone in the fight against COVID-19, but precautions must still be taken to prevent the spread of the virus. As Dr. Walensky said, “We must remain vigilant. Nobody wants to see the patient readmitted to the hospital.”
As Covid-19 continues to ravage countries across the globe, the World Health Organization (WHO) has announced the end of the Public Health Emergency of International Concern (PHEIC) for the disease. However, this is not an indication that the pandemic has ended, but rather that it has shifted from an emergency phase to an endemic one. The move is a recognition of the fact that the virus is unlikely to be eradicated, and that it may become a permanent part of the infectious diseases that societies must manage, like the flu.
To understand the decision, it is important to look at the trends in the numbers. The end of January 2020 saw the first PHEIC declaration by the WHO, when no deaths had been reported in the US. Since then, there have been almost 9,900 new hospital admissions related to Covid-19 in the US for the week ending May 1, and around 1,050 deaths per week at the end of April. As a medical professional, the author stresses that while absolute numbers are important, trends are more significant in understanding the course of an illness.
Downward Trend
The decision to end Public Health Emergency (PHE) status in the US may appear premature, given the nearly 9,900 new Covid-related hospital admissions and 1,050 deaths per week. But in medicine, trends tell a richer, more complete story than absolute numbers alone. In this case, while cases, hospitalizations, and deaths are still high, they are moving in the right direction. This trend applies globally and prompted WHO’s decision to end the PHEIC declaration. However, WHO would not hesitate to declare a new global health emergency if necessary.
The philosophical question that arises is how much Covid-related sickness and death societies are willing to tolerate to avoid disruptions to daily life. It’s a question public health and other experts have grappled with for three years. The answer comes down to the number of Covid deaths societies can accept in exchange for restoring normalcy.
If the US maintained its weekly death rate at the end of April for an entire year, Covid would cause around 54,700 deaths annually, comparable to a bad influenza season. However, effective public health strategies, such as wearing high-quality masks and improving indoor ventilation, can only do so much. Social responsibility and collective action are also necessary.
“The pandemic continues to pose a severe threat, but hope is on the horizon,” said Dr. Tedros of WHO. Vaccines have the power to control Covid but require global access to be an effective solution.
“The biggest risk we face now is complacency. People are tired, and understandably so. But we cannot give up. We must continue to do everything we can to save lives,” Tedros added.
Given this state of affairs, it is essential to remember that while the end of PHE calls for cautious optimism, the virus is likely to remain endemic in the long term. Experts recommend prioritizing vaccine access, implementing effective public health strategies, and continuing to monitor trends to prevent future outbreaks.
“We can’t just flip the switch and declare victory over a virus that isn’t done with us yet. This shift in the pandemic may feel sudden, but it’s been a long time coming,” says Dr. Sauers-Ford, a public health expert. “We need to remain vigilant to prevent future spikes in cases, hospitalizations, and deaths.”
Doctor’s Orders on Moving Forward
As we come to the close of this pandemic chapter, it is important to remember that there are still many Americans who are concerned about contracting Covid-19, especially those who are older and sicker. According to the CDC, the risk of hospitalization for those 75 and older is 9 to 15 times higher than for those who are 18 to 29. Additionally, people with pre-existing conditions, such as asthma, hypertension, chronic kidney disease, or severe obesity, have a higher risk of severe illness and hospitalization.
The pandemic has underscored the importance of good health, and the United States’ collective poor health put us at a disadvantage. While we had resources to fight the pandemic, we must focus on improving our overall health. “No amount of wealth can buy good health,” as Dr. Sanjay Gupta, a neurosurgeon and CNN’s Chief Medical Correspondent, writes.
As people begin to venture out of the hospital and back into the world, it is essential to remember a few precautions. If you are sick, stay at home. Talk to your doctor about keeping a course of oral antivirals, such as Paxlovid, in your medicine cabinet if you are at higher risk of hospitalization or death. According to Dr. Anthony Fauci, “If you are vaccinated and boosted and have available therapy, you are not going to die [of Covid], no matter how old you are.” This should be reassuring for people, especially those in their 80s or older.
Furthermore, it is crucial to take care of your health to feel better, happier, and stronger now and in the future. Invest in yourself by adopting healthy habits such as eating well, exercising, and engaging in activities that promote mental and physical well-being.
Despite the challenges posed by the pandemic, we have found ways to adapt, learn, and grow. We can use this experience as a launching point for personal growth and make conscious decisions that support our well-being and that of others.
Dr. Gupta writes, “I wish my patient well. I wish us all well.” Let us move forward with a renewed commitment to our health and well-being.
“True and Total Health is the Wellbeing of Mind, Body, and Spirit” will be the theme for the 41st annual Convention 2023 of the American Association of Physicians of Indian Origin (AAPI) planned to be held at the iconic Marriott Downtown in Philadelphia, PA from July 6th-9th, 2023” Dr. Ravi Kolli, President of AAPI announced during a press meet on April 25, 2023.
The virtual press conference was addressed by Dr. Ravi Kolli, President of AAPI, Dr. V. Ranga, Chair of AAPI Board of Trustees, Dr. Satheesh Kathula, Vice President of AAPI, Dr. Meher Medavaram, Secretary of AAPI, Dr. Sumul Raval, Treasurer of AAPI, and Dr. Sreeni Gangasani, CME Chair, who has been newly elected as the Treasurer-Elect of AAPI.
Dr. Kolli informed the media that AAPI successfully concluded its annual election with the participation of over 5,000 members to elect a new leadership team that will be taking charge at the convention. Headed by Dr. Anjana Samadder, the only 5th woman president of AAPI in its 41 years long history, the new team will comprise of Dr. Satheesh Kathula as the President-Elect, Dr. Amit Chakrabarty as the Vice President, Dr. Sumul Raval as the Secretary; Dr. Sreeni Ganagasani as the Treasurer; and Lokesh Edara – as the Chair, Board of Trustees.
Dr. Ravi Kolli will continue to serve AAPI as the Immediate Past President of AAPI and help the leadership in their tasks as needed. In response to a question on his tenure as president of AAPI, Dr. Kolli said “I maintained good relations with everyone, every group, every region, and everybody. I am very proud of my contributions in bringing people together and reaching out to team members to reach their with full potential.”
While describing the schedule for the three-day convention, Dr. Kolli said, the convention will be addressed by eminent speakers, including Indian- American Congressmen, Ro Khanna, Raja Krishnamoorthi, and Ami Bera, and Congresswoman Pramila Jayapal as well as senators, Governors of Pennsylvania and New Jersey. Mika Singh will perform at the convention along with other artists, and Miss England will also attend as a special guest.
Additionally, Spiritual guide of Heartfulness Meditation and Padma Bhushan awardee, Kamlesh Patel commonly known as Daaji, Her Holiness Jagadguru Sai Ma, representatives from Bochasanwasi Akshar Purushottam Swaminarayan Sanstha (BAPS), and other spiritual institutions have been invited. CME speakers and faculty from prestigious institutions including U Penn, Harvard and Stanford will also participate in the convention, AAPI president Ravi Kolli informed.
Dr. Kolli said that the event will host panel discussions on the future of health care, CEO forums, and sessions on artificial intelligence and emerging technologies in conjunction with entertainment and cultural sessions.
According to Dr. Ranga, “The American Association of Physicians of Indian Origin Convention offers an exciting venue to interact with leading physicians, health professionals, academicians, and scientists of Indian origin. Physicians and healthcare professionals from across the country will convene and participate in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities in the coming year.”
“AAPI Convention will focus on addressing physician burnout and the Convention team has planned several wellness packages,” said Dr. Anjana Samadder, President-Elect of AAPI. “As we witness a significant increase in physician burnout, Convention will be an opportunity to relax, interact with your colleagues, and learn effective ways to address the challenges in caring for patients and care for self and thus avoid burn out,” Dr. Samadder added.
“Our Annual Convention in Philadelphia is just around the corner. Our team is working very hard with great enthusiasm, and they are all very excited to see you in this fantastic memorable event. Some of the highlights of the convention are: Very informative CMEs, product theaters; Women’s Forum, CEO Forum, Financial Seminars, Spiritual sessions &Yoga, Obesity awareness walk, Alumni reunions, Local Tours, Special programs for non-physician spouses, and lots more,” said Dr. Raghunandan Lolabhattu, CEO & Acting Chair of Convention 2023 and Vice Chair of Board of Trustees, AAPI.
“We will have one of the very best conventions in history,” Dr. Kathula said. “The convention will focus on Mental Health as well as Physical health and various other medical specialty updates, Dr. Sanjay Gupta, Convener of the Convention stated that “Medical Jeopardy, Research, and Poster presentations by medical students, will be a great way to bring the next generation of physicians into AAPI and will help accomplish the mission of AAPI. In addition, advocacy to dismantle the stigma of mental illness and Suicide Prevention will be the highlight of the program.”
While describing the many initiatives of AAPI both in India and the United States over the past four decades, Dr. Medavaram said, “The American Association of Physicians of Indian Origin Convention offers an exciting venue to interact with leading physicians, health professionals, academicians, and scientists of Indian origin. Physicians and healthcare professionals from across the country will convene and participate in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities in the coming year.”
Dr. Raval said, “The scientific program, comprising of CMEs and workshops at the convention are developed by leading experts with contributions from the Scientific Advisory Board and the International Scientific Committee. The workshops will be led by world-famous physicians on topics relevant to the needs of the time.” Discussions and deliberations will address the Stigma of Mental illness, Suicide prevention, Management of Chronic diseases and NCD and, other health issues including Climate Change and its impact on health will be discussed, he added.
Dr. Gangasani referred to some of the topics for the CMEs will include Psychiatry, Ophthalmology, Pediatrics, Gastroenterology, Neurology, and Oncology. “In our efforts to realize the core mission of AAPI, which is to share the best from leading experts from around the world, to collaborate on clinical challenges, the convention will have clinical tracks that are of vital to healthcare leaders and members,” Dr. Gangasani added.
While urging all AAPI members to make plans and be part of the historic Convention, Dr. Kolli said: “We have a wonderful team planning and organizing the event to make the 2023 annual convention a memorable experience. Please reach out to any one of the representatives from the Philly team for any of your queries and visit www.aapiconvention.org for more details or call the AAPI office at (630) 990 2277 for further information.
The Biden administration has issued a warning to Americans concerning the financial risks associated with medical credit cards and other loans for medical bills. In a recent report, the Consumer Financial Protection Bureau (CFPB) estimated that Americans paid $1 billion in deferred interest on medical credit cards and other medical financing between 2018 and 2020. The agency found that interest payments can increase medical bills by almost 25 percent, which can deepen patients’ debts and threaten their financial security.
CFPB’s Director, Rohit Chopra, stated that “lending outfits are designing costly loan products to peddle to patients looking to make ends meet on their medical bills. These new forms of medical debt can create financial ruin for individuals who get sick.” Nationally, KFF Health News found that approximately 100 million people, including 41 percent of adults, have healthcare debt. This large scale problem is feeding a multibillion-dollar patient financing business, with private equity and big banks looking to capitalize on the situation when patients and their families are unable to pay for care. The profit margins in the patient financing industry top 29 percent, according to research firm IBISWorld, which is seven times what is considered a solid hospital profit margin.
One of the most prominent financing options is credit cards like CareCredit offered by Synchrony Bank which is often marketed in physician and dentist waiting rooms to help pay off medical bills. These cards typically offer a promotional period where patients pay no interest, but if the patient missed a payment or could not pay off the loan during the promotional period, they could face interest rates that rise as high as 27 percent, according to the CFPB. Patients are also increasingly drawn into loans administered by financing companies such as AccessOne.
These loans, which often replace no-interest instalment plans that hospitals once commonly offered, can add hundreds or thousands of dollars in interest to the debts patients owe. Hospital and finance industry officials insist that they take care to educate patients about the risks of taking out loans with interest rates. However, federal regulators have found that many patients remain confused about the terms of the loans.
According to the CFPB, the risks are particularly high for lower-income borrowers and those with poor credit. About a quarter of people with a low credit score who signed up for a deferred-interest medical loan were unable to pay it off before interest rates jumped. By contrast, just 10% of borrowers with excellent credit failed to avoid the high interest rates. Regulators found that many patients remained confused about the terms of the loans and that patients often didn’t fully understand the products’ terms and found themselves in crippling financing arrangements.
Despite this, the new CFPB report does not recommend new sanctions against lenders. The study cautioned that the system still traps many patients in damaging financing arrangements. It also stated that “consumers complain that these products offer confusion and hardship rather than benefit, as claimed by the companies offering these products.” The report concluded that “many people would be better off without these products.”
The growth of patient financing products pose risks to low-income patients. Patients should be offered financial assistance to pay large medical bills, but instead, they are funnelled into credit cards, debt consolidations or personal loans that pile interest on top of medical bills they cannot afford.
An investigation conducted by KFF Health News with NPR explored the scale and impact of the nation’s medical debt crisis. They found that 41% of adults have some form of healthcare debt. In the patient financing industry, profit margins are over 29%, which is nearly 7x higher than what is considered to be a solid hospital profit margin. A UNC Health public records analysis found that after AccessOne began administering payment plans for the system’s patients, the percentage of people paying interest on their bills increased from 9% to 46%.
According to the CFPB, “Patients appear not to fully understand the terms of the products and sometimes end up with credit they’re unable to afford.” Federal regulators warned that patient financing products pose another risk to low-income patients. They should be offered financial assistance with large medical bills, but instead, they are being routed into credit cards or loans that pile interest on top of medical bills they cannot afford.
Medical credit cards and other loans for medical bills can deepen patients’ debts and threaten their financial security. The number of people with healthcare debts is increasing, and many patients remain confused about the terms of the loans. Profit margins in the patient financing industry are high, and patients are often funnelled into credit cards rather than offered financial assistance with large medical bills. This can lead to confusion and financial ruin for those who get sick. The report concluded that “many people would be better off without these products.”
The US Food and Drug Administration (FDA) has granted approval for a new vaccine that can help fight respiratory syncytial virus (RSV), an illness that leads to the death of thousands of people each year in America. The vaccine, named Arexvy by the UK-based manufacturer GSK, has been hailed as a significant breakthrough that could save many lives. However, it still needs evaluation from the US Centers for Disease Control and Prevention (CDC) before it can be made available to the public.
Dr Peter Marks, who leads the Center for Biologics Evaluation and Research at the FDA, said, “Today’s approval of the first RSV vaccine is an important public health achievement to prevent a disease which can be life-threatening.”
RSV is a respiratory disease that typically causes cold-like symptoms for adults. However, it can prove dangerous for young children, those with underlying health conditions, and older adults aged over 65 who suffer from the virus. On average, it kills between 100 and 300 children under the age of 5 in America every year, and causes between 6,000 to 10,000 fatalities among adults over 65 annually, leading to between 60,000 to 120,000 hospitalisations.
According to the CDC, the quickest way to prevent RSV is through vaccination. Arexvy is the first vaccine capable of preventing RSV anywhere in the world, having been in development for over 60 years. Arexvy has an efficacy rate of 82.6%, according to a study by GSK in February.
The most common side effects are “mild or moderate,” such as discomfort around the injection site or fatigue, typically subsiding within two days. Officials say the vaccine could be available to people aged over 60 within the next few months.
Dr Susanna Naggie, an infectious disease specialist, at Duke University School of Medicine, in Durham, North Carolina said, “This is a very important and long-awaited advance for an infection that causes significant morbidity and mortality, particularly in older adults.”
The breakthrough vaccine could potentially save numerous lives, and its approval by the FDA is a critical step in the fight against RSV.
Recognizing the Signs of Respiratory Syncytial Virus (RSV) in Children
RSV typically begins with a stuffy or runny nose, followed by a dry cough, fever, and occasionally, difficulty breathing. In most cases, it is mild and can be managed with infant paracetamol or ibuprofen. If your child is not drinking enough fluids, having difficulty breathing or has a temperature that won’t go down, consult your doctor or seek medical attention. If your little one is having trouble breathing to the point of exhaustion – muscles around their ribs are prominently drawing in as they take each breath and they are pale and sweaty – immediately call emergency services.
A year into the pandemic, the impact on physicians varied based on specialties, personal experiences and geography. But physicians now face staffing shortages, anti-science aggression, incivility and new dimensions of moral distress. These factors have contributed to a sharp increase in the burnout rate to 63% this year, compared to previous years. Professional fulfilment, on the other hand, refers to the sense of satisfaction and enjoyment that emanates from work.
Between Dec. 9, 2021, and Jan. 24, 2022, nearly 2,500 U.S. physicians responded to a survey conducted by researchers from the AMA, the Mayo Clinic, Stanford University School of Medicine and the University of Colorado School of Medicine. Their findings were alarming, with professional fulfilment scores dropping from 40% in 2020 to a mere 22.4% in 2021.
The study says that “At the organization level, a number of randomized and controlled trials as well as systematic reviews and meta-analyses have reported that organizational interventions both work and are critical to creating an organizational culture and practice environment that cultivates professional fulfilment”.
In light of the reported decline in professional fulfillment and increased burnout among physicians, here are six ways to make a difference and improve joy and meaning in work:
Build Resilient Health Systems
Resilient health systems support and protect the individuals within. To address the systemic drivers of physician burnout and support the full spectrum of professional fulfillment and well-being, it is important to use feedback from physicians to drive meaningful changes, have critical conversations and track progress.
Measure the State of Staff Well-being
Ochsner performs an “Organizational Biopsy™,” which includes a burnout assessment and an expanded set of questions across key domains of organizational culture, practice efficiency and individual self-care. This allows leaders to identify drivers of professional fulfillment and assess issues such as intent to reduce work hours or leave the organization at granular department and service-line levels, while also benchmarking against other health systems.
Ease In-Basket Burden to Restore Joy in Medicine
The pandemic led to a 57% increase in patient medical advice requests via inbox messages, and the increased work demands have become the new normal for physicians. This added workload has cut into physicians’ time, and each message adds an extra 2.32 minutes of EHR active-use time while also contributing to physician burnout. Some organizations have found ways to ease this in-basket burden to restore joy in medicine. For instance, Atrius Health was able to cut the inbox volume by 25% for primary care physicians who previously received about 100 messages daily.
Gain Insight into an Organization
A chief wellness officer (CWO) can help an organization systematically improve and maintain the well-being of physicians and other health professionals. However, before implementing changes, it is important for the CWO to study and understand the organization.
Improve Organizational Culture
To reduce burnout, interventions like advanced models of team-based care with in-room support can improve practice efficiency. At the same time, interventions to improve organizational culture, including connections with colleagues and improved local leadership, can improve professional fulfillment and reduce burnout.
Focus on Joy and Meaning in Medicine
Achieving joy and meaning in medicine is essential, especially in today’s context. Organizations aiming to help physicians and other health professionals attain joy and meaning in medicine need to focus on improving operational efficiency and care experience.
Reducing physician burnout remains a critical component of the AMA Recovery Plan for America’s Physicians. The AMA develops resources that prioritize well-being and highlight workflow changes so physicians can focus on what matters: patient care. “It’s critical that we address this issue now so that we can rebuild the health care workforce and maintain access to care for millions of Americans,” said Susan R. Bailey, MD, president of the AMA.
Tamil Nadu, India’s southernmost state, hosted a two-day medical value travel conclave on Saturday and Sunday, April 29-30th, 2023, which was inaugurated by Chief Minister M.K. Stalin. The conclave, titled “Tamil Nadu – Where the World Comes to Heal,” was aimed at bringing together accredited hospitals from Tamil Nadu with hospitals from 21 source countries. The event was jointly organized by the Tourism and Health departments.
The medical value travel sector is worth $25 billion globally and is growing rapidly. Patients from other countries come to India, either referred by hospitals or via agents. However, the sector is not very organised and needs streamlining. Around 80 representatives from hospitals listened to experts in 10 specialties, including plastic surgery, gastroenterology, cancer, and heart and lung transplant. The hospitals included those under the Ayush Ministry, and a session on holistic healing was also held.
The conclave included a B2B session where hospital representatives met each other without the interference of agents. A special secretariat would be set up to keep in touch with foreign hospitals, and meetings like this would be held annually, according to Tourism Secretary B. Chandra Mohan.
“Through this conclave, we hope to promote Tamil Nadu as a destination for medical value travel. The state has a wealth of qualified medical professionals and state-of-the-art hospitals, making it an ideal location for medical tourists,” said Mohan.
The event was attended by Ministers Ma. Subramanian, K. Ramachandran, T. M. Anbarasan, and T. Mano Thangaraj, Health Secretary P. Senthilkumar, and Director of Tourism Sandeep Nanduri, according to a press release.
In his speech, Chief Minister M.K. Stalin said, “Medical tourism can provide a significant boost to our state’s economy, and we must work together to ensure that we provide the best possible care to our patients.”
Overall, the conclave was a great success, bringing together hospitals from around the world and promoting Tamil Nadu as a destination for medical value travel. With the medical value travel sector growing rapidly, it is important to streamline the sector and provide the best possible care to patients.
Unlocking the Power of Your Senses: Enhancing Happiness, Productivity, and Relationships with Gretchen Rubin’s ‘Life in Five Senses
A decade ago, the author Gretchen Rubin embarked on a personal journey to find ways to lead a happier life. Through rigorous scientific research and testing the wisdom of the ages, she learned several ways of improving relationships, boosting energy, and other techniques that lead to a fulfilling life. However, years later, she realized she was disconnected from other people and herself. After introspection, she realized that she was treating her body as a vehicle driven by the brain rather than a means to connect with the world through the senses.
During the exploration that led to the book “Life in Five Senses,” the author discovered how the senses could help people focus on living happier, more productive lives. She found that different senses under different circumstances could bring calmness, creativity, higher awareness, energy, and more.
The World Health Organization (WHO) declared on Friday that Covid-19 is no longer a global health emergency; a decision reached after the International Health Regulations Emergency Committee discussed the pandemic at its 15th meeting on the virus. WHO Director-General Tedros Adhanom Ghebreyesus confirmed that the public health emergency of global concern, or PHEIC, declaration should end, stating that “for more than a year the pandemic has been on a downward trend”. However, while Covid-19 remains a threat, the virus is evolving, and the WHO has said it would not hesitate to convene another emergency committee meeting and declare a global health emergency again if there was a significant rise in Covid-19 cases or deaths in the future.
Picture : KFF
A PHEIC creates an agreement in which countries abide by the WHO’s recommendations for managing the emergency. Each country then makes its own public health emergency declaration, declarations that carry legal weight. Countries use them to marshal resources and waive rules to ease a crisis. However, Dr. Maria Van Kerkhove, WHO’s Covid-19 technical lead and head of its program on emerging disease, said that the emergency phase of the Covid-19 crisis is over, but the disease is “here to stay” and the coronavirus that causes the disease is not going away anytime soon, as cases are expected to continue to occur epidemiologically.
Dr. Mike Ryan, the Executive Director of WHO’s Health Emergencies Programme, noted: “There’s still a public health threat out there, and we all see that every day in terms of the evolution of this virus, in terms of its global presence, its continued evolution and continued vulnerabilities in our communities, both societal vulnerabilities, age vulnerabilities, protection vulnerabilities, and many other things”.
While the pandemic appears to be decreasing, Covid-19 cases and deaths remain significant, with more than 765 million confirmed cases worldwide and nearly seven million people dead. Europe has had the most confirmed cases overall, but the Americas have reported the most deaths, approximately 1 in 6 of all total deaths being American. Cases reached their highest rate in December 2022 as Omicron swept the globe, hitting the Western Pacific significantly. However, billions of vaccine doses have already been administered globally, and deaths have remained far below previous peaks.
Tedros has emphasised that Covid-19 “has left and continues to leave deep scars on our world” and that these should be a permanent reminder of the potential for new viruses to emerge with devastating consequences. Tedros also highlighted that “one of the greatest tragedies of Covid-19 is that it didn’t have to be this way. We have the tools and technologies to prepare for pandemics better, detect them earlier, respond to them faster, and communicate their impact. But globally, a lack of coordination, a lack of equity, and lack of solidarity meant that those tools were not used as effectively as they could have been”. He went on to stress the importance of developing better preparedness and coordination for any future global health emergencies.
There remains a global disparity in vaccine distribution, with billions of people unvaccinated and at risk of contracting Covid-19, and officials continue to warn against complacency and the need to maintain vigilance in managing the pandemic. Van Kerkhove said “While we’re not in the crisis mode, we can’t let our guard down. Epidemiologically, this virus will continue to cause waves. What we are hopeful of is that we have the tools in place to ensure that the future waves do not result in more severe disease, don’t result in waves of death and we can do that with the tools we have at hand”.
While Covid-19 is no longer considered a global health emergency by the WHO, the virus remains a threat, and the need for preparedness, collaboration, and vaccine distribution to manage future waves of the pandemic are crucial. As the world struggles to emerge from the pandemic, officials warn that complacency is not an option and that vigilance is needed to protect lives, reduce transmission, and prevent future pandemics.
Loneliness and social isolation have become prevalent issues that are affecting the mental and physical health of Americans, according to a warning from the surgeon general issued on Tuesday. The advisory is the first of its kind to address the problem of loneliness. It points out a 2021 poll that found more than half of Americans are lonely, with young adults twice as likely to feel isolated as those over 65.
Surgeon General Dr. Vivek H. Murthy, who has written a book on the subject “Together: The Healing Power of Human Connection in a Sometimes Lonely World,” is calling for the country to strengthen its social fabric by prioritizing meaningful relationships. Dr. Murthy advises that everyone can benefit from rebuilding and cultivating connections with others, regardless of whether they consider themselves lonely or not. In light of this, he has offered some practical advice on addressing loneliness.
Dr. Murthy emphasizes the importance of acknowledging loneliness as a normal and prevalent experience. In seeking solutions, he encourages people to build up their support networks by prioritizing relationships and setting aside time for socializing. He advises setting realistic expectations when making connections, accepting that building strong relationships takes time and effort.
Dr. Murthy also recommends that people take steps to develop deeper connections through activities that involve shared interests and values. Social media can be helpful in fostering existing relationships, but Dr. Murthy recommends focusing on in-person interactions whenever possible. In conclusion, he emphasizes that loneliness affects everyone differently, and that there is no one-size-fits-all solution to the problem of social isolation. However, by taking steps to strengthen our social bonds, we can all benefit from the healing power of human connection.
Nurture Relationships
Maintaining healthy relationships is a vital part of our lives. Whether it is familial or platonic, relationships require nurturing. Dr. Vivek H. Murthy, former Surgeon General of the United States, recommends taking 15 minutes each day to connect with a friend or family member. Dr. Murthy suggests putting a reminder in your calendar as a helpful tool to make this a priority.
“Those brief in-person interactions can make us feel good for a long time because we are hard-wired to connect,” says Dr. Murthy.
Dr. Murthy advises people to “be real” when conversing with others. You do not have to pretend to be someone you are not, just be the real you. At first, this might be scary, but remember that people are wired to connect. Sharing honestly and inviting others to reciprocate can be “incredibly powerful,” according to Dr. Murthy. Remember, your relationships need nurturing to thrive, so take time to connect with your loved ones.
Put Down Your Devices and Focus on In-Person Communication
Cell phones have the ability to distract us from personal interactions and reduce the quality of our relationships. It is important to give people our full attention, and to listen attentively to what they have to say. According to a recent report, despite the rise of social media, Americans report having fewer friends than they had in the past. This decrease in social connection has been attributed to disconnected communication caused by technology.
In-person communication enables the exchange of more than just words, but also allows for the exchange of nonverbal cues and a deeper experience of connection. It is important to remember to put down cell phones, reduce use of social media, and provide full attention while communicating in person to create more meaningful relationships.
“Over thousands of years we evolved to not only understand the content of what someone was saying but also to respond to the tone of their voice, to read their body language, and to experience their presence,” said Dr. Murthy, emphasizing the importance of face-to-face communication.
Don’t Ignore Calls, Pick Up and Talk
Imagine receiving a call from your college best friend whom you haven’t talked to for a while. However, instead of picking up, you decline the call, intending to call back later when you have enough time to talk.
Next time, Dr. Murthy said, pick up the phone and talk. If you’re in the middle of something, say, “Hey, it’s really good to hear your voice,” and then find another time to talk.
“That 10 seconds feels so much better than going back and forth on text,” he said.
Volunteering for Others Can Help Combat Loneliness
According to research, volunteering can alleviate loneliness and expand our social connections. You could contribute your time to a local organization or offer assistance to your family, colleagues, or acquaintances.
“When we help other people we establish an experience or a connection with them — but we also remind ourselves of the value that we bring to the world,” Dr. Murthy said. “And that’s essential because when people struggle with loneliness over time, it does erode their self-esteem and their sense of self. It can make them believe over time that they’re lonely because they’re not likable or they’re not lovable. And when we serve others, we come to see that that’s not the case.”
Seek Assistance
If you are experiencing loneliness, do not hesitate to confide in a family member, friend, therapist, or healthcare provider. Additionally, if persistent feelings of sadness and hopelessness are disrupting your daily routines and hindering your participation in activities you enjoy, seeking professional help is crucial. Having thoughts of harming yourself is a serious issue that requires immediate attention, so use the 988 crisis hotline for assistance.
“Continuing the excellent efforts to help their motherland by the members of the American Association of Physicians of Indian Origin (AAPI), building on the successful program, ADOPT-A-VILLAGE with the goal of adopting 75 Villages in India, commemorating India’s 75th Independence Day, AAPI has signed a Memorandum of Understanding with Doctors of Rajasthan International (DORI) to carry out screenings in five villages initially in the state of Rajasthan, and hoping to have several additional villages,” Dr. Ravi Kolli, President of AAPI announced here today.
Present during the MOU signing ceremony were prominent DORI members from across the globe, including Drs. Jaivir Rathore, Brahma Sharma, Ranvir Singh Rathore, AAPI EC including Drs. Ravi Kolli, Anupama Gotimukula, Satheesh Kathula, and President and CEO of GTC, Dr. Radha Ramana Murthy Gokula.
While India has made substantial progress in health care as evidenced by the fact that life expectancy in India at birth now is 71 years as opposed to 58 years in 1990 and 41 years in 1960, there are significant gaps and divergences in health metrics in different regions in India.
Picture : TheUNN
India needs to redouble and continue its efforts and dedicate resources to tackle these perennial challenges. The post-graduate training of physicians specializing in Family Medicine in every teaching institution will create motivated and well-trained family physicians to address these deficits and deliver accessible, affordable, economical, and continuous preventive and primary care to rural as well as urban poor populations to raise health outcomes across India.
Realizing the need to bridge this gap, AAPI has launched this much-needed and popular ADOPT-A-Village Program, chaired by, Dr. Satheesh Kathula, the current Vice President of AAPI. while Dr. Anupama Gotimukula, Dr. Jagan Ailinani and Dr. Murthy Gokula serve as members of the Committee.
AAPI has embarked on free screening for NCDs in 75 villages to commemorate 75 years of India’s independence. The screening tests include CBC, HbA1C, lipid profile, creatinine, pulse oximetry, measurement of blood pressure, height, and weight.
To date, through the efforts of AAPI and its local organizers in these states, over 8,0000 patients in several states across India including Andhra Pradesh, Gujarat, Himachal Pradesh, Jharkhand, Karnataka, and Telangana have been screened. Now with an MOU Rajasthan, people in this state will have an opportunity to screen a few thousand more in rural India.
AAPI initiated the Digital Integrated Prevention And Management Program (DIPAM), a Rural Health Initiative in India in a virtual launch event on Gandhi Jayanthi on October 2nd, 2022. The data collected from the screenings has been very interesting which will help the Health Officials in India establish a preventive health task force in India. AAPI in partnership with Global Teleclinics (GTC) is currently working on a Digital Integrated Prevention and Management (DIPAM) program with the vision of raising awareness of disease management and reversal of NCDs to improve healthcare outcomes by connecting rural India with medical providers and other partners.
Dr. Anupama Gotimukula, Immediate Past President of AAPI referred to the goals of Adopt-A-Village. “As India celebrates her 75th anniversary of Independence Day, AAPI has been working on adopting 75 villages across India in several states, where the rural people of India are being offered ‘Free Health Screenings in 75 Villages, for Anemia (CBC), DM (HbA1C), High Cholesterol, CKD, Malnutrition, Obesity, and Hypoxemia. Results are being analyzed by GTC, and further treatment plans are recommended by their team of experts with follow-ups. This is a small contribution by AAPI to Mother India in celebration of Azadi Ka Amrut Mahotsav.”
Dr. Satheesh Kathula, Chairman of AAPI’s Adopt a Village Program pointed out the need for this noble initiative. He said, “India has nearly 700,000 villages, where 77 percent of the poor live. The majority of the population has no access to basics such as safe drinking water and healthcare. “By adopting one village at a time and working with the government and NGOs, NRIs can make a huge difference,” he said.
Dr. Kathula referred to the rural initiative as “A much-needed project to prevent silent killers such as Hypertension, diabetes, Hypercholesterolemia, and chronic kidney disease. Adopt A Village program also helped rural India with the supply of cloth masks, and clean drinking water and has helped thousands of people across India. We are excited about providing continuous healthcare in India with DIPAM.”
Dr. Brahma Sharma said, “By adopting one village at a time and working with the government and NGOs, NRIs can make a huge difference in the lives of millions of people in India. Each project will involve a tripartite partnership between the NRI, state government, and a local NGO.”
Dr. Murthy Gokula, President of Global Teleclinics said, “Adopt-A-Village is a great opportunity to enhance the effectiveness of telehealth through awareness, education, and sustainable development in all villages.”
The project is aimed at bringing Non-Communicable Diseases (NCDs) screening and prevention to rural people at their doorsteps of India and raising awareness of disease management and reversal of Non-Communicable Diseases to improve health outcomes and connect rural India with medical providers and partners.
Initially launched with the goal to adopt and screen 75 villages for: Hypertension, Diabetes, Anemia, Chronic Kidney disease, and Hyperlipidemia, the phase 2 project aims at providing: in person complete physical exam for positive NCD patients every 3 months; Giving 3-month medications for the identified illnesses; Daily teleclinic through the app-based solution; Communication with the villagers through WhatsApp or telephone; Access to a local health care worker hired by global teleclinics for daily interaction and emergencies; and, Utilize local medical resources: RMPs, PHC personnel for immediate care,
While there is no instant solution for rural India’s myriad problems, by adopting one village at a time, and working with the government and NGOs, NRIs can make a difference, and over time, an improved village could lead to an improved region, state, and country.
Dr. Kolli thanked the AAPI members for their generous support of this noble work of AAPI and for sponsoring their ancestral villages. Dr. Kolli urged “AAPI members to consider joining this movement and adopt a village. Maybe your own village of origin. AAPI will work with you in coordinating the efforts and through the support system we have in several states, will help you achieve this goal of giving back to our motherland.” AAPI members/families can sponsor a Village by emailing: aapipresident@aapiusa.org and info@aapiusa.org. For more details, please visit www. aapiusa.org
Researchers at the Grossman School of Medicine at NYU have discovered new evidence as to why human hair loses its natural colour over time, which they believe can also be applied to preventing the greying of human hair. The study examined the melanocyte stem cells (McSCs) that control hair colour, and found that earlier in life, these cells can be remarkably dynamic. However, with age, these cells tend to slow down, getting trapped in what is known as the hair follicle bulge, meaning they do not get a chance to finish the job they were created to do. Reinforcing these cells could mean the end of grey hair, according to the team at NYU.
“The newfound mechanisms raise the possibility that the same fixed positioning of melanocyte stem cells may exist in humans. If so, it presents a potential pathway for reversing or preventing the graying of human hair by helping jammed cells move again,” said study leader, Qi Sun,a postdoctoral fellow at NYU Langone Health
Lab mice that had their hair “physically aged” by plucking and forced regrowth were observed to have a 15% higher concentration of McSCs stuck in that follicle bulge before their hairs were pulled. Following the intervention, the percentage of hairs that no longer had pigment generating abilities rose to nearly 50%. With the greater understanding of the stalled-out cells and their probable responsibility for loss of hair colour, researchers are now focusing on how to get the McSCs back on track.
The next research step will be “to investigate means of restoring motility of McSCs or of physically moving them back to their germ compartment, where they can produce pigment,” according to lead researcher Professor Mayumi Ito,PhD
Dr Doris Day, a dermatologist affiliated with Lenox Hill Hospital in New York City, commented that although the new study is interesting and needed, it is still “early days” for any human hair solution.
Walking after a meal has long been considered a beneficial habit for clear thinking and improved digestion. However, it has been discovered that even small amounts of walking, for as little as two to five minutes, can activate benefits, particularly reducing blood sugar levels. A recent meta-analysis published in the journal Sports Medicine looked at seven studies that examined the effects of walking versus sitting or standing on heart health. The studies showed that light walking after a meal can improve blood sugar levels, which is particularly helpful in warding off Type 2 diabetes.
Dr. Kershaw Patel, a preventive cardiologist at Houston Methodist Hospital, who was not involved in the study, says that “each small thing” you do will have benefits.
For example, light walking almost instantly impacts blood sugar levels, especially when done within 60-90 minutes after eating a meal. This can make a significant difference in minimizing blood sugar spikes. Walking during this time can reduce the risk of developing Type 2 diabetes because sharp spikes and crashes in blood sugar levels are thought to contribute to developing the condition.
Very light walking reduces blood sugar levels
The seven studies that examined walking versus sitting or standing showed that light walking improves blood sugar levels compared to sitting at a desk or lounging on the couch. When participants walked even for short amounts of time, their blood sugar levels rose and fell more gradually. For people with diabetes, sharp fluctuations in blood sugar levels can be particularly problematic, making it more important for them to stabilize their levels. Those with pre-diabetes or Type 2 diabetes can benefit from walking, as spikes and troughs in blood sugar levels can contribute to a higher risk of developing the disease.
Walking within 60 to 90 minutes after eating delivers the best results.
Standing also helps lower blood sugar levels, but it does not have the same degree of impact as light walking. Standing has some benefits, but the researchers found “light-intensity walking was a superior intervention.” Light walking challenges muscles and uses fuel from food circulating in the bloodstream, reducing excess glucose in the muscles. Jessie Inchauspé, author of the book Glucose Revolution: The Life-Changing Power of Balancing Your Blood Sugar, says that “your muscles will soak up some of that excess glucose,” indicating that light walking helps reduce the impact of a meal on the body.
Mini-walks are more practical during the workday
Aidan Buffey, a graduate student at the University of Limerick in Ireland and author of the research paper, recommends a mini-walk of two to three minutes during a workday. It is more practical to perform during the workday, and people are more likely to engage in this activity than to go for a run. Buffey suggests getting up to make coffee, walk down the hallway or take a stroll after lunch. These activities can lead to measurable changes, as shown in the studies, and will enhance other dietary changes that people may be making to improve their blood sugar levels.
Dr. Euan Ashley, a cardiologist at Stanford University, who was not associated with the study, says “moving even a little bit is worthwhile.” He provides a continuum concept of incremental benefits that show each step or walk seems to have a benefit. Dr. Patel agrees with this concept and indicates that the benefits of physical activity exist on a continuum. He notes that “it’s a gradual effect of more activity, better health.”
Taking a small walk after a meal can benefit those who want to stabilize blood sugar levels, which is especially important for people with diabetes and for those who want to avoid developing it. Walking for just two to five minutes after a meal can make a difference in comparison to sitting at a desk or lounging on the couch. For the most significant impact on stabilizing blood sugar levels, taking a short walk within 60 to 90 minutes of eating is the most effective. A mini-walk of two to three minutes during a workday is more practical and feasible for most people, which makes it an excellent option to improve overall health.
Indian diet rich in iron, zinc, and fibre, regular consumption of tea, and use of turmeric in meals lowered severity and death due to Covid in the country, according to a study published in the April edition of the Indian Journal of Medical Research by the Indian Council of Medical Research (ICMR).
During the Covid-19 pandemic, the death rate was reportedly 5-8 fold lower in India which is densely populated as compared to lesser-populated western countries.
The study, conducted by an international team of scientists including from India, Brazil, Jordan, Switzerland, and Saudi Arabia, aimed to investigate whether dietary habits were associated with the variations in Covid-19 severity and deaths between Western and Indian population.
“Our results suggest that Indian food components suppress cytokine storm and various other severity-related pathways of Covid-19 and may have a role in lowering severity and death rates from Covid-19 in India as compared to western populations,” said the researchers including from Centre for Genomics and Applied Gene Technology at Institute of Integrative Omics & Applied Biotechnology, in West Bengal, and Policy Center for Biomedical Research at Translational Health Science & Technology Institute in Haryana.
“However, large multi-centered case-control studies are required to support our current findings,” they added. The findings showed that the components of Indian diets, which maintain high iron and zinc concentrations in blood and rich fibre in foods, played a role in preventing carbon dioxide (CO2) and lipopolysaccharide (LPS)-mediated Covid-19 severity.
LPS is a common inflammatory mediator to induce inflammatory processes in the brain.
Further, regular consumption of tea by Indians helped maintain high HDL (high-density lipoprotein), also called “good” cholesterol. The catechins in tea also acted as a natural atorvastatin (a statin medication used to prevent cardiovascular diseases) in lowering triglyceride in blood.
Importantly, they said, regular consumption of turmeric in daily food by Indians led to a strong immunity. The curcumin in turmeric may have prevented pathways and mechanisms associated with SARS-CoV-2 infection and Covid-19 severity and lowered the death rate, said the researchers.
On the other hand, increased consumption of red meat, dairy products and processed foods resulted in an increase in the severity and death due to Covid in the western populations.
These foods “activate cytokine storm-related pathways, intussusceptive angiogenesis, hypercapnia and enhance blood glucose levels due to high contents of sphingolipids, palmitic acid and by-products such as CO2 and LPS” they wrote in the study.
Palmitic acid – the most common saturated fatty acid found in the human body – also induces ACE2 expression and increases the infection rate, the team said.
Coffee and alcohol that are highly consumed in western countries also led to an increase in severity and death rates from Covid-19 by deregulating blood iron, zinc and triglyceride levels.
For the study, the team used blood transcriptomes of severe Covid-19 patients from three western countries (showing high fatality) and two datasets from Indian patients.
Gene set enrichment analyses were performed for pathways, metabolites, nutrients, etc., and compared for Western and Indian samples to identify the food- and nutrient-related factors, which may be associated with Covid-19 severity.A
Data on the daily consumption of twelve key food components across four countries were collected and a correlation between nutrigenomics analyses and per capita daily dietary intake was also investigated. (IANS)
Dr. Dattatreyudu Nori, a world renowned Indian-American oncologist, has been appointed as the senior advisor to the Chennai-center of the Memorial Sloan Kettering Cancer Center from New York. The Padma Shri awardees was named one of the top doctors in America for the treatment of cancers, especially in women. Memorial Sloan Kettering Cancer Center (MSKCC), a cancer treatment and research institution in the borough of Manhattan in New York City is one of the world’s top cancer centers.
Picture : TheUNN
The center’s Chennai facility is its first overseas center, which opened last year. Dr. Nori stated that the opening of the center in India is a big deal and aims to bring the best practices of cancer treatment from the United States to India. He also emphasized the importance of providing the best treatment for cancer patients. The center’s presence in India will help to increase awareness in the fight against the deadly disease and save a large number of lives.
Speaking to the media, Nori said that he gets a lot of patients from India whom he treats at MSKCC. He noted that Indian patients look out for different hospitals and opinions, and they spend a lot of money going to different centers before reaching MSKCC. And therefore, he had aimed to have one of its centers open in India.
According to him the India centre will make a second opinion option available to Indians within the country, eliminating the need to travel to the US. Nori emphasized that the first treatment for cancer cure should be the best. “There is no room for catching up,” the doctor said.
A MSKCC centre was opened in Chennai, India in 2020. However, Nori mentioned that good cancer centers are coming up in the country in the last ten years, but they are not able to cater to the needs of all cancer patients. He recommended the Indian government to focus on controlling the incidents of cancer through screening and early detection. The doctor is also trying to introduce new programs in India that were successful in the US.
Speaking on the importance of early screening, Nori said that in the US it has reduced the occurrence of cervical cancer by 24 per cent, mammography has reduced the mortality of breast cancer, and awareness programs about smoking caused a downward trend of lung cancer. He revealed that he will be introducing some of these programs in India.
The Padma Shri awardee who hails from Andhra Pradesh obtained his medical degree from Kurnool Medical College and a postgraduate degree from Osmania Medical College. He is known for the development and application of brach.
Newswise — People who live in countries with more stringent alcohol policies drank less than people in countries with less strict policies, according to a large multi-country analysis published in Alcohol: Clinical and Experimental Research. The more stringent policies were associated with reduced drinking overall and showed more significant associations in drinkers aged 18 to 24 and those with 13 or fewer years of education. The findings suggest that countries could reduce adverse health consequences by adopting cost-effective alcohol policies.
The researchers investigated whether the International Alcohol Control (IAC) Policy Index is associated with drinking patterns in the overall population and specific demographic groups in a diverse set of countries. The IAC Policy Index measures the implementation and enforcement of policies shown by previous studies to be cost-effective in reducing alcohol use, namely policies restricting alcohol availability, marketing, pricing, and drinking and driving. In this study, researchers examined the strength of these policies in ten diverse countries to determine each country’s International Alcohol Control Policy (IAC) score. The higher the IAC score, the stronger the country’s alcohol policies are. Drinkers in each country were surveyed about drinking behaviors, including frequency, quantity, and locations of alcohol consumption.
The study found that the IAC score was significantly associated with the volume and frequency of drinking in the ten countries, with greater interaction in certain demographic groups. Overall, with each additional increase in the IAC score, the average volume of alcohol consumed in the prior six months decreased by 17 percent, and the frequency of drinking decreased by 14 percent. By age group, young adults aged 18 to 24 showed the largest decrease in alcohol consumed on a typical occasion. In countries with less restrictive alcohol policies, this age group shows the highest quantity of alcohol consumption.
There was also an association between stronger policies and drinking quantity by education level. In countries with weaker alcohol control policies, those with less education drank more on each occasion than those with more than 13 years of schooling. As alcohol policies strengthened, the number of adults with less education who drank per occasion decreased to levels similar to those of more educated respondents.
By gender, men’s and women’s consumption decreased as the IAC score increased, but men’s consumption decreased more slowly than women’s.
More than 17,000 people across ten countries participated in the study. The countries participating in the study included five high-income and five middle-income countries, namely New Zealand, England, Australia, Scotland, South Africa, St. Kitts and Nevis, Mongolia, Thailand, Vietnam, and Turkey, with IAC scores ranging from 5 for New Zealand to 13.9 for Turkey. The study focused on the most effective policies and did not measure the possible influence of other policies or cultural traditions on respondents’ behaviors.
India’s population growth rate on a steady decline since ’90s
According to the UNFPA (United Nations Population Fund), India’s population in 2021 stood at 1,393.4 million with an average annual rate of change of population of 1%
(Chicago, IL: April 16, 2023) “Congratulations and best wishes to the new team of AAPI leadership, who have been elected to lead AAPI in the coming years,” Dr. Ravi Kolli, President of AAPI, and Chief Election Officer Dr. Kusum Punjabi and Past BOT Chair of AAPI, jointly announced here today. “We thank the election officers Dr. Ashok Jain, Dr. Sunita Kanumury, Dr. Sharad Lakhanpal, and Dr. Shashi Shah, and all the members of AAPI for participating in the democratic election process and exercising their role as the electoral college members.”
While thanking the tens of thousands of Indian American physicians, who are active members of the American Association of Physicians of Indian Origin (AAPI), and the record number of large number voters who participated in the election process, Dr. Kolli said, “We have successfully concluded our elections for the year 2023-24 for AAPI leadership positions. We want to thank AAPI members who enthusiastically participated in the AAPI’s electronic voting process and have elected a new, diverse, balanced, and experienced team to lead AAPI, the largest ethnic medical organization in the United States in the coming year and beyond.”
Picture : TheUNN
Dr. Kusum Punjabi, Chief Election Officer – 2023, who along with the election committee conducted the elections and counting process in the virtual presence of all the candidates and their representatives communicated the results of the election to the AAPI president to be released to all the members of AAPI and noted that Dr. Amit Chakrabarty has been elected as the Vice President of AAPI, Dr. Sumul Raval was elected as the Secretary, and Dr. Sreeni Gangasani was elected Treasurer of AAPI for the year 2023-24.
Dr. Syamala Erramilli, Dr. Hetal Gor, and Dr. Narendra Maheshwari have been elected to the AAPI’s Board of Trustees for a three-year term. Dr. Vijay Gunuganti has been elected as the South West Central Regional Director of AAPI, and Dr. Anuradha Mann will be the new Regional Director of AAPI’s South East Central Region.
“As the incoming President of AAPI, I would like to congratulate my incoming new team for the fiscal year 2023-24,” said Dr. Anjana Samadder, who will assume charge as the President of AAPI during the 41st annual convention in Philadelphia, PA in July this year. “I’m very honored and consider myself fortunate to be bestowed with the responsibility of leading the four-decades-old strong organization with the cooperation and collaboration of an excellent team of dedicated, hardworking, and loyal officers and executive committee members who are with me to take AAPI to newer heights,” she added.
Dr. Sammader did not have to contest the election this year, as she has been serving as the President-Elect during the past year. Dr. Satheesh Kathula, who has been serving as the Vice President in the current year also did not have to face elections, as he automatically becomes the President-Elect of AAPI for the coming year.
Dr. Anjana Samadder, the only 5th woman president of AAPI in its 41 years long history, will have a dynamic and diverse team comprising of Dr. Satheesh Kathula as the President-Elect, Dr. Amit Chakrabarty as the Vice President; Dr. Sumul Raval as the Secretary; Dr. Sreeni Ganagasani as the Treasurer; and Dr. Lokesh Edara – as the Chair, Board of Trustees; Dr. Ravi Kolli will continue to guide AAPI as the Immediate Past President of AAPI.
Dr. Lokesh Edara will serve as the Chair of the AAPI Board of Trustees for the year, 2023-24. “As the BOT Chair, I am looking forward to working towards strengthening the goals and mission of AAPI and to help make AAPI a healthcare leader in the US and globally and work in the best interests of our Physicians and our community here in the US and serve our motherland, India,” said Dr. Edara. “We will work together to promote our values of professionalism, collegiality, and excellence in patient care and enhance AAPI’s reputation as a premier professional organization offering educational programs and advocacy.”
While congratulating the newly elected leaders to the Executive Committee, Dr. Kathula, the President-Elect in 2023-24 said here in a statement: “I want to congratulate all the winners of the election. I want to especially thank all the candidates for their passion and dedication to serving AAPI and regardless of the outcome, we need you as a valuable team member of our beloved AAPI.”
Dr. Amit Chakrabarty, who won the election to be the next Vice President of AAPI, said, “I am humbled and honored to be bestowed with this responsibility. Thank you all for your support and for making my 25 years quest come true. I thank all for believing in me. I will work to the fullest of my abilities to reach our goals, address the challenges, and advance the issues important to our members. I look forward to working with you and making AAPI a powerful force. I am a live example that dreams do come true with dogged perseverance, dedication, and loyalty to AAPI.”
Dr. Sumula Raval, Secretary-Elect of AAPI said, “It is with great joy and gratitude that I stand before you today as the newly elected Secretary of AAPI for the year 2023-2024. I am humbled by the overwhelming support and trust you have placed in me, and I am deeply honored to serve this esteemed organization in such a significant role. I am committed to building upon past achievements and leading AAPI with integrity, transparency, and innovation. I will focus on promoting diversity and inclusion in healthcare, advocating for the needs of our members, and fostering collaboration. Let us continue to work hand in hand to make a positive impact on healthcare and uphold the values of AAPI.”
Dr. Sreeni Gangasani, the newly elected Treasurer of AAPI said, “I am thrilled and deeply humbled to have been elected as AAPI Treasurer for 2023-24. It is an honor to have your trust and confidence in me to help manage the finances of this fantastic organization. I promise to uphold the highest standards of transparency, accountability, and integrity in managing our finances. I will work to ensure that our resources are used effectively to further our mission of promoting excellence in patient care, research, and education. I am excited about the opportunities that lie ahead for our organization.”
Dr. V. Ranga, the outgoing BOT Chair thanked the Election Committee for their meticulous planning and organizing the elections with integrity and fairness. He said, “I congratulate the winners and the new leadership who are entrusted with the responsibility of leading AAPI in the year 2023-24 and beyond. I wish them the very best and my wholehearted support.”
While conceding the election to Dr. Amit Chakrabarty to be the next Vice President of AAPI, Dr. Krishan Kumar said, “Thank you so much for supporting me all these years. I am glad to see the healthy spirit of all candidates (winners or not) for the association.” In his message, Dr. Raj Bhayani, while conceding the election said, “I am thankful to my supporters who gave me their precious vote honoring my many years of service for AAPI.”
Dr. Sujeeth Punnam in his message to the elected leaders, said, “Congrats to all the winners. We sacrifice time from family, practice, and resources to work in this great organization. The only reward is the ultimate feeling that we are contributing to the greater good of Indian physicians in the US and humankind in general. I wish Dr. Sumul Raval the best of luck as he moves forward with his new responsibility.” Dr. Mukesh Nigam in his congratulatory note to Dr. Gangasani and all the winners, said, “I will continue to serve this great association, AAPI. AAPI is a big family full of talented people. I cherish every moment of being part of it.”
The growing influence of physicians of Indian heritage is evident, as increasingly physicians of Indian origin hold critical positions in healthcare, academic, research, and administrative positions across the nation. We the physicians of Indian origin are proud of our great achievements and contributions to our motherland, India, our adopted land, the US, and in a very significant way to the transformation of Indo-US relations.
Serving 1 in every 7 patients in the US, AAPI members care for millions of patients every day, while several of them have risen to hold high-flying jobs, shaping the policies and programs, and inventions that shape the landscape of healthcare in the US and around the world.
“Since its inception in 1982, AAPI has been at the forefront, representing a conglomeration of more than 125,000 practicing physicians in the United States, seeking to be the united voice for the physicians of Indian origin. I trust and believe that the new Team under Dr. Anjana Samadder will continue the noble mission and strengthen our efforts to make AAPI reach greater heights,” said Dr. Ravi Kolli. For more details about AAPI, please visit: www.appiusa,org
The Biden administration is expanding federal health care services to Deferred Action for Childhood Arrivals (DACA) program recipients. According to a White House statement, the Department of Health and Human Services will shortly propose a rule amending the definition of “lawful presence,” for purposes of Medicaid and Affordable Care Act coverage, to include DACA recipients.
DACA recipients often referred to as Dreamers are eligible immigrants who came to the United States as children dependent on their parents’ work visas. While they have grown up and received their education in America they are not recognised as U.S. citizens or lawful permanent residents. The program does not grant them official legal status or a pathway to citizenship.
Picture : Idaho Capital sun
According to the statement, President Biden believes that the Dreamers strengthen U.S economy, and enrich schools and the community. His administration’s proposed plan will allow Dreamers to apply for coverage through the health insurance marketplace and through the state Medicaid agency just like other citizens.
“We are not done fighting for their pathway to citizenship, but we’re getting them the opportunities they deserve in the meantime,” Biden said making the historic announcement.
The democratic government aims to protect and strengthen the federal health insurance agencies by lowering costs and expanding coverage so that every American has the peace of mind that health insurance brings and the inclusion of DACA recipients is a step in that direction.
“The Administration continues to urge Congress to provide a pathway to citizenship to Dreamers, providing them the ultimate peace of mind they need and deserve,” the White House statement emphasized.
At present, schemes and programs available to DACA recipients include; AmeriCorps VISTA Program (to assist local organizations in alleviating poverty), a range of outdoor programming, environmental education, and volunteer service programs, and American job centers to help job seekers obtain employment and training to further their careers.
The vaccine technology America learned about during the pandemic was originally aimed at cancer, but its use against infectious diseases took off in the pandemic. Now a new study suggests specially designed mRNA shots can help prevent recurrences of melanoma, a dreaded skin cancer.
The study, presented Sunday at a research conference, showed that after nearly two years, patients who received a personalized mRNA vaccine made by Moderna and Merck were 44% more likely to be alive and avoid new tumors than those who received only the standard of care.
If the results hold up in a larger, longer study planned to start later this year, it will mark a dramatic turnaround for cancer vaccines, which have been tested and failed for decades.
“It’s probably the first real data that suggests that this personalized approach to vaccination may be worth exploring further,” said Dr. Ryan Sullivan, an oncologist at Mass General Cancer Center, who was a co-author on the study.
Instead of using a vaccine to try to prevent or shrink a tumor, the new mRNA vaccines are aimed at reducing the chances of a high-risk cancer recurring.
“This represents a big shift in how we’re using cancer vaccines,” said Dr. Robert Vonderheide, who was not involved in the study but is the program committee chair of the American Association for Cancer Research’s annual meeting, where the study was presented.
The pandemic proved that mRNA vaccines, already in development for cancer, could be used safely and developed quickly, said Vonderheide, who also directs the Abramson Cancer Center at the University of Pennsylvania.
Benefits seen in melanoma, a cancer known to be controlled by the immune system, are likely to hold up in other cancers that are affected by the immune system, he and several other experts said. The next one to be tested will be non-small-cell lung cancer, which kills about 100,000 Americans a year.
But it made sense to try first in melanoma.
“No cancer is as immunotherapy sensitive as melanoma is,” said Dr. Rodabe Amaria, a melanoma oncologist at MD Anderson Cancer Center in Houston, who was not involved in the study. “You have to prove it in melanoma before you try it in other cancers.”
How would an mRNA cancer vaccine work?
These vaccines are designed to prevent cancer recurrences, not an initial run-in with the disease.
After surgical removal of a tumor or a separate biopsy, scientists send a sample of tissue and blood for genetic sequencing, looking for proteins that are unique to the cancer and not present in healthy tissue.
The mRNA vaccine is then designed to target 34 of these distinctive proteins, getting the immune system to recognize them and hopefully kill the cells that make them without damaging healthy tissue.
Because there are so many possible neoantigens, resulting from a patient’s own genetics and the evolution of their tumor cells, the vaccine must be bespoke, designed specifically for each person.
Researchers aren’t sure how many neoantigens to target or which are likely to offer the most benefit, “so we cram in as many potential neoantigens as possible,” said Dr. Eliav Barr, chief medical officer of Merck, which supported the trial.
Each vaccine takes about eight weeks to manufacture and is based on tumor cells removed during surgery. While the patient waits for their personalized vaccine, they start taking the drug pembrolizumab (brand name Keytruda), made by Merck, which unleashes the immune system to attack cancer.
Pembrolizumab is given as a 30-minute infusion every three weeks for a year. Patients receive two or three doses of pembrolizumab and then, when their vaccine is ready, they get nine doses along with their next nine infusions, before completing pembrolizumab.
According to findings released Sunday by the researchers, but not yet peer reviewed, among 107 volunteers who received both the experimental vaccine and pembrolizumab, the cancer returned in 24 (22%) within two years. There were 20 recurrences (40%) among the 50 people who received only pembrolizumab.
(Keytruda sells for a list price of $185,000 a year, although most people will not pay the list price, according to Merck. It’s too soon to know how much companies will charge for mRNA vaccines.)
Melanoma is diagnosed in about 100,000 Americans per year. If caught early, nearly everyone survives for at least five years, but only one-third of patients whose cancer has spread widely survive that long.
“Pembro” already dramatically decreased recurrences, but the new study showed a 44% extra benefit with the addition of the mRNA vaccine, called mRNA-4157/V940.
“We’re already reaping those benefits (from pembro), and now, in such a short period of time to have an additional therapeutic agent that builds on that progress is a very exciting thing,” Amaria said.
Side effects of mRNA vaccine for cancer
The addition of the mRNA vaccine did not seem to add substantially to the side effects already seen with pembrolizumab.
Pembro often affects the endocrine system, Amaria said, causing diabetes and potentially permanent thyroid problems. Other common side effects include exhaustion, muscle pain, rash, diarrhea, fever, cough, decreased appetite, itching, shortness of breath, constipation and nausea.
As more patients live longer with melanoma, these side effects are becoming more noticeable, Amaria said. “In some patients, the benefit goes hand-in-hand with the toxicity,” so side effects may be a sign the treatment is working.
“In some patients, we’re fundamentally changing their quality of life,” she said, but “most people do have normal lives, recovered from side effects.”
What is mRNA?
Messenger RNA carries instructions from a cell’s DNA code to the cellular machinery that manufactures proteins, telling it what to make. Delivered as a vaccine, the short-lived mRNA turns cells into factories that produce desired proteins.
With COVID, mRNA vaccines produce the spike protein found on the surface of the SARS-CoV-2 virus, training the immune system to recognize and wipe out viral cells.
In the case of these cancer vaccines, the mRNA triggers the body to produce the 34 neoantigens, training the immune system to recognize and target them.
In cancers that have spread beyond an initial tumor, surgeons can’t remove all the cancerous cells. In people with Stage 2 melanoma or above, this dangerous spread has already begun and the risk of recurrence after surgery is very high.
The vaccine should help prevent these dangerous recurrences, Barr said.
The mRNA vaccine can’t be used to prevent disease, as it is with COVID, because the neoantigens don’t exist until the tumor does, Barr said. But it appears to work well when designed to target a specific person’s cancer and hopefully providing long-term memory, so even future cancer cells will be killed.
BioNTech, the German company that helped develop the other mRNA vaccine against COVID, is also working on cancer vaccines, including against ovarian and lung cancer, as are several other companies.
It’s not really clear why an mRNA vaccine would be effective against cancer when so many other approaches have failed, several experts said. The technology may simply spur more reaction from tumors, Sullivan said.
What happens next?
The new study, launched in 2018, was relatively small and only lasted a few years, so Merck hopes to start a large, Phase 3 trial later this year. It will be open to people with Stage 2 or Stage 3 melanoma.
Amaria said she and her colleagues at MD Anderson are considering participating. Patients often come to her asking for an mRNA vaccine against their cancer, she said.
Dr. Jeffrey Weber, who led the new study and is the deputy director of the Perlmutter Cancer Center at NYU Langone, said he’s optimistic about the future of mRNA vaccines against cancer.
“It’s got a ways to go, but I do believe that these results will hold up over time,” he said.
The Huanan seafood and wildlife market in China has been a focal point in the search for the origin of the coronavirus that has impacted the world as none other in the past three years. People around the world have been seeking to identify the origin of the deadly virus.
Now a research team in China has published analysis of samples taken more than three years ago from the market linked to the outbreak of Covid-19. This is the first peer-reviewed study of biological evidence gathered from the market back in 2020.
By linking the virus with animals sold in the market, it could open new lines of inquiry into how the outbreak began. The research reveals swabs that tested positive for the virus also contained genetic material from wild animals.
Some scientists say this is further evidence that the disease was initially transmitted from an infected animal to a human. But others have urged caution in interpreting the findings and it remains unclear why it took three years for the genetic content of the samples to be made public.
The Chinese research team posted an early version of their study online back in February 2022, but they did not publish the full genetic information that was contained in the samples gathered from the market.
This new analysis, which has been validated by other scientists before being published in the journal Nature, includes more important detail about the content of those samples, which were collected from stalls, surfaces, cages and machinery inside the market. Before the 2020 outbreak, scientists took photos of animals, including racoon dogs, being sold in the Huanan market
The Chinese research team’s paper showed that some samples – collected from areas where wildlife was being sold – had tested positive for the virus. Their analysis also showed that animals now known to be susceptible to the virus, particularly raccoon dogs, were being sold alive in those locations.
But the Chinese researchers have pointed out that their discoveries fall short of definitive proof of how the outbreak started. “These environmental samples cannot prove that the animals were infected,” the paper explains. The possibility remains, it adds, that the virus was brought into the market by an infected person, rather than an animal.
Prof David Robertson, from the University of Glasgow, is a virologist who has been involved in the genetic investigation into the origin of SARS-CoV-2 since it emerged in 2020. He told BBC News: “The most important thing is that this very important dataset is now published and available for others to work on.”
But he added that the contents of the samples were “compelling evidence that animals there were probably infected with the virus. It’s the whole body of evidence that’s important,” he said. “When you bring this together with the fact that the early Covid-19 cases in Wuhan are linked to the market, it’s strong evidence that this is where a spillover from an animal in the market occurred.”
According to BBC, the published findings come amid signs that the lab leak theory is gaining ground among authorities in the US. The Chinese government has strenuously denied suggestions that the virus originated in a scientific facility, but the FBI said it now believes that scenario is the “most likely”, as does the US Department of Energy.
Various US departments and agencies have investigated the mystery and produced differing conclusions, but on March 1st, the FBI’s director accused Beijing of “doing its best to try to thwart and obfuscate”, and disclosed the bureau had been convinced of the lab leak theory “for quite some time now”.
The FBI has not made their findings public, which has frustrated some scientists. The lead researcher of the new report, from the Chinese Center for Disease Control and Prevention (China CDC) in Beijing, has been contacted by the BBC for comment.
Northwestern University researchers have discovered a previously unknown mechanism that drives aging. In a new study, researchers used artificial intelligence to analyze data from a wide variety of tissues, collected from humans, mice, rats, and killifish. They discovered that the length of genes can explain most molecular-level changes that occur during aging.
All cells must balance the activity of long and short genes. The researchers found that longer genes are linked to longer lifespans, and shorter genes are linked to shorter lifespans. They also found that aging genes change their activity according to length. More specifically, aging is accompanied by a shift in activity toward short genes. This causes the gene activity in cells to become unbalanced.
Surprisingly, this finding was near universal. The researchers uncovered this pattern across several animals, including humans, and across many tissues (blood, muscle, bone, and organs, including liver, heart, intestines, brain, and lungs) analyzed in the study.
The new finding potentially could lead to interventions designed to slow the pace of — or even reverse — aging. The study was published December 9 in the journal Nature Aging.
“The changes in the activity of genes are very, very small, and these small changes involve thousands of genes,” said Northwestern’s Thomas Stoeger, who led the study. “We found this change was consistent across different tissues and in different animals. We found it almost everywhere. I find it very elegant that a single, relatively concise principle seems to account for nearly all of the changes in activity of genes that happen in animals as they age.”
“The imbalance of genes causes aging because cells and organisms work to remain balanced — what physicians denote as homeostasis,” said Northwestern Engineering’s Luís A.N. Amaral, a senior author of the study. “Imagine a waiter carrying a big tray. That tray needs to have everything balanced. If the tray is not balanced, then the waiter needs to put in extra effort to fight the imbalance. If the balance in the activity of short and long genes shifts in an organism, the same thing happens. It’s like aging is this subtle imbalance, away from equilibrium. Small changes in genes do not seem like a big deal, but these subtle changes are bearing down on you, requiring more effort.”
An expert in complex systems, Amaral is the Erastus Otis Haven Professor of Chemical and Biological Engineering at the McCormick School of Engineering. Stoeger is a postdoctoral scholar in Amaral’s laboratory.
Looking across ages
To conduct the study, the researchers used various large datasets, including the Genotype-Tissue Expression Project, a National Institutes of Health-funded tissue bank that archives samples from human donors for research purposes.
The research team first analyzed tissue samples from mice — aged 4 months, 9 months, 12 months, 18 months, and 24 months. They noticed the median length of genes shifted between the ages of 4 months and 9 months, a finding that hinted at a process with an early onset. Then, the team analyzed samples from rats, aged 6 months to 24 months, and killifish, aged 5 weeks to 39 weeks.
It seems that, at a young age, our cells are able to counter perturbations that would lead to an imbalance in gene activity. Then, suddenly, our cells are no longer able to counter it. Thomas Stoeger Postdoctoral Scholar, Northwestern University
“There already seems to be something happening early in life, but it becomes more pronounced with age,” Stoeger said. “It seems that, at a young age, our cells are able to counter perturbations that would lead to an imbalance in gene activity. Then, suddenly, our cells are no longer able to counter it.”
After completing this research, the researchers turned their attention to humans. They looked at changes in human genes from ages 30 to 49, 50 to 69 and then 70 and older. Measurable changes in gene activity according to gene length already occurred by the time humans reached middle age.
“The result for humans is very strong because we have more samples for humans than for other animals,” Amaral said. “It was also interesting because all the mice we studied are genetically identical, the same gender and raised in the same laboratory conditions, but the humans are all different. They all died from different causes and at different ages. We analyzed samples from men and women separately and found the same pattern.”
‘Systems-level’ changes
In all animals, the researchers noticed subtle changes to thousands of different genes across samples. This means that not just a small subset of genes that contributes to aging. Aging, instead, is characterized by systems-level changes.
This view differs from prevailing biological approaches that study the effects of single genes. Since the onset of modern genetics in the early 20th century, many researchers expected to be able to attribute many complex biological phenomena to single genes. And while some diseases, such as hemophilia, do result from single gene mutations, the narrow approach to studying single genes has yet to lead to explanations for the myriad changes that occur in neurodegenerative diseases and aging.
“We have been primarily focusing on a small number of genes, thinking that a few genes would explain disease,” Amaral said. “So, maybe we were not focused on the right thing before. Now that we have this new understanding, it’s like having a new instrument. It’s like Galileo with a telescope, looking at space. Looking at gene activity through this new lens will enable us to see biological phenomena differently.”
Lengthy insights
After compiling the large datasets, many of which were used in other studies by researchers at Northwestern University Feinberg School of Medicine and in studies outside Northwestern, Stoeger brainstormed an idea to examine genes, based on their length.
The length of a gene is based on the number of nucleotides within it. Each string of nucleotides translates to an amino acid, which then forms a protein. A very long gene, therefore, yields a large protein. And a short gene yields a small protein. According to Stoeger and Amaral, a cell needs to have a balanced number of small and large proteins to achieve homeostasis. Problems occur when that balance gets out of whack.
Although the researchers did find that long genes are associated with increased lifespans, short genes also play important roles in the body. For example, short genes are called upon to help fight off pathogens.
“Some short genes could have a short-term advantage on survival at the expense of ultimate lifespan,” Stoeger said. “Thus, outside of a research laboratory, these short genes might help survival under harsh conditions at the expense of shortening the animal’s ultimate lifespan.”
Suspected ties to long COVID-19
This finding also may help explain why bodies take longer to heal from illnesses as they age. Even with a simple injury like a paper cut, an older person’s skin takes a longer time to recover. Because of the imbalance, cells have fewer reserves to counteract the injury.
“Instead of just dealing with the cut, the body also has to deal with this activity imbalance,” Amaral hypothesized. “It could explain why, over time with aging, we don’t handle environmental challenges as well as when we were younger.”
And because thousands of genes change at the system-level, it doesn’t matter where the illness starts. This could potentially explain illnesses like long COVID-19. Although a patient might recover from the initial virus, the body experiences damage elsewhere.
“We know cases where infections — predominantly viral infections — lead to other problems later in life,” Amaral said. “Some viral infections can lead to cancer. Damage moves away from the infected site and affects other areas of our body, which then is less able to fight environmental challenges.”
Hope for medical interventions
The researchers believe their findings could open new venues for the development of therapeutics, designed to reverse or slow aging. Current therapeutics to treat illness, the researchers argue, are merely targeting the symptoms of aging rather than aging itself. Amaral and Stoeger compare it to using Tylenol to reduce a fever instead of treating the illness that caused the fever.
“Fevers can occur for many, many reasons,” Amaral said. “It could be caused by an infection, which requires antibiotics to cure, or caused by appendicitis, which requires surgery. Here, it’s the same thing. The issue is the gene activity imbalance. If you can help correct the imbalance, then you can address the downstream consequences.”
Other Northwestern co-senior authors include Richard Morimoto, a professor of molecular biosciences in the Weinberg College of Arts and Sciences; Alexander Misharin, an associate professor of medicine at Feinberg; and G.R. Scott Budinger, the Ernest S. Bazley Professor of Airway Diseases at Feinberg and chief of pulmonary and critical care at Northwestern Medicine.
Amusement and pleasant surprises — and the laughter they can trigger — add texture to the fabric of daily life. Those giggles and guffaws can seem like just silly throwaways. But laughter, in response to funny events, actually takes a lot of work, because it activates many areas of the brain: ones that control motor, emotional, cognitive and social processing.
People begin laughing in infancy, when it helps develop muscles and upper body strength. Laughter is not just breathing. It relies on complex combinations of facial muscles, often involving movement of the eyes, head and shoulders.
Laughter — doing it or observing it — activates multiple regions of the brain: the motor cortex, which controls muscles; the frontal lobe, which helps you understand context; and the limbic system, which modulates positive emotions. Turning all these circuits on strengthens neural connections and helps a healthy brain coordinate its activity.
Laughing with others helps to create social bonds and can increase intimacy.
By activating the neural pathways of emotions such as joy and mirth, laughter can improve your mood and make your physical and emotional response to stress less intense. For example, laughing may help control brain levels of the neurotransmitter serotonin, similar to what antidepressants do. By minimizing your brain’s responses to threats, it limits the release of neurotransmitters and hormones such as cortisol that can wear down your cardiovascular, metabolic and immune systems over time. Laughter’s kind of like an antidote to stress, which weakens these systems and increases vulnerability to diseases.
Laughter’s cognitive power
A good sense of humor and the laughter that follows depend on an ample measure of social intelligence and working memory resources.
Laughter, like humor, typically sparks from recognizing the incongruities or absurdities of a situation. You need to mentally resolve the surprising behavior or event — otherwise you won’t laugh; you might just be confused instead. Inferring the intentions of others and taking their perspective can enhance the intensity of the laughter and amusement you feel.
To “get” a joke or humorous situation, you need to be able to see the lighter side of things. You must believe that other possibilities besides the literal exist — think about being amused by comic strips with talking animals, such as those found in “The Far Side.”
Laughter’s social power
Many cognitive and social skills work together to help you monitor when and why laughter occurs during conversations. You don’t even need to hear a laugh to be able to laugh. Deaf signers punctuate their signed sentences with laughter, much like emoticons in written text.
Laughter creates bonds and increases intimacy with others. Linguist Don Nilsen points out that chuckles and belly laughs seldom happen when alone, supporting their strong social role. Beginning early in life, infants’ laughter is an external sign of pleasure that helps strengthen bonds with caregivers.
Later, it’s an external sign of sharing an appreciation of the situation. For example, public speakers and comedians try to get a laugh to make audiences feel psychologically closer to them, to create intimacy.
By practicing a little laughter each day, you can enhance social skills that may not come naturally to you. When you laugh in response to humor, you share your feelings with others and learn from risks that your response will be accepted/shared/enjoyed by others and not be rejected/ignored/disliked.
In studies, psychologists have found that men with Type A personality characteristics, including competitiveness and time urgency, tend to laugh more, while women with those traits laugh less. Both sexes laugh more with others than when alone.
Laughter’s mental power
Positive psychology researchers study how people can live meaningful lives and thrive. Laughter produces positive emotions that lead to this kind of flourishing. These feelings — such as amusement, happiness, mirth and joy — build resiliency and increase creative thinking. They increase subjective well-being and life satisfaction. Researchers find that these positive emotions experienced with humor and laughter correlate with appreciating the meaning of life and help older adults hold a benign view of difficulties they’ve faced over a lifetime.
Laughter in response to amusement is a healthy coping mechanism. When you laugh, you take yourself or the situation less seriously and may feel empowered to problem-solve. For example, psychologists measured the frequency and intensity of 41 people’s laughter over two weeks, along with their ratings of physical and mental stress. They found that the more laughter experienced, the lower the reported stress. Whether the instances of laughter were strong, medium or weak in intensity didn’t matter.
Maybe you want to grab some of these benefits for yourself — can you force laughter to work for you?
A growing number of therapists advocate using humor and laughter to help clients build trust and improve work environments; a review of five different studies found that measures of well-being did increase after laughter interventions. Sometimes called homeplay instead of homework, these interventions take the form of daily humor activities — surrounding yourself with funny people, watching a comedy that makes you laugh or writing down three funny things that happened today.
You can practice laughing even when alone. Intentionally take a perspective that appreciates the funny side of events. Laughing yoga is a technique of using breathing muscles to achieve the positive physical responses of natural laughing with forced laughter (ha ha hee hee ho ho).
Researchers today certainly aren’t laughing off its value, but a good deal of the research on laughter’s influence on mental and physical health is based on self-report measures. More psychological experimentation around laughter or the contexts in which it occurs will likely support the importance of laughing throughout your day, and maybe even suggest more ways to intentionally harness its benefits. (Courtesy: https://www.cnn.com/2023/04/01/health/laughter-mind-body-wellness-partner/index.html)
Depression is defined by the American Psychological Association as intense melancholy or despair that lasts longer than days. It disrupts daily activities and may result in physical symptoms including discomfort, weight gain or loss, irregular sleeping patterns, or a lack of vitality.
The World Health Organization (WHO) estimates that 264 million people are affected by depression, making it the biggest cause of disorder globally. Psychologists polled for the 2020 APA study claim that more people have come out to ask for professional advice and assistance over the course of the pandemic. Even while being acknowledged by many, this disorder is still stigmatized highly and is often misunderstood for being lazy or inactive in certain activities.
The myths associated with depression are also something to look out for. “It’s unimportant,” “simply snap out of it,” sadness just affects women, “talking or thinking about the same would only make the problem worse,” and “all emotions related with sad circumstances are part of being depressed.” Just as we see there are lot of misconceptions and misleading facts about the same. People need to do a lot of study and understand the topic of concern before labeling something on themselves and each other.
Regardless of age, gender, or social situation, anyone can develop depression. Several aspects, including as heredity, trauma, persistent stress, and drug usage, might also be involved. The symptoms associated with it could be mixed feelings of sadness, hopelessness, worthiness, and the difficulty to perform everyday activities, lose of interest in activities once enjoyed, changes in appetite and sleep pattern, and thoughts in suicide.
The first step towards any healing is to ask for help, and then proceeding towards taking on the treatments, like therapy, medication, and lifestyle changes from exercises, healthy eating habits to stress reduction techniques. It is also advised to seek professional help.
Newswise — Cold activates a cellular cleansing mechanism that breaks down harmful protein aggregations responsible for various diseases associated with aging. In recent years, studies on different model organisms have already shown that life expectancy increases significantly when body temperature is lowered.
However, precisely how this works has still been unclear in many areas.
A research team at the University of Cologne’s CECAD Cluster of Excellence in Aging Research has now unlocked one responsible mechanism.
The study ‘Cold temperature extends longevity and prevents disease-related protein aggregation through PA28γ-induced proteasomes’ has appeared in Nature Aging.
Professor Dr David Vilchez and his working group used a non-vertebrate model organism, the nematode Caenorhabditis elegans, and cultivated human cells. Both carried the genes for two neurodegenerative diseases which typically occur in old age: amyotrophic lateral sclerosis (ALS) and Huntington’s disease. Both diseases are characterized by accumulations of harmful and damaging protein deposits – so-called pathological protein aggregations. In both model organisms, cold actively removed the protein clumps, thus preventing the protein aggregation that is pathological in both ALS and Huntington’s disease.
More precisely, the scientists explored the impact of cold on the activity of proteasomes, a cellular mechanism that removes damaged proteins from cells. The research revealed that the proteasome activator PA28γ/PSME3 mitigated the deficits caused by aging in both the nematode and in the human cells. In both cases, it was possible to activate proteasome activity through a moderate decrease in temperature. “Taken together, these results show how over the course of evolution, cold has preserved its influence on proteasome regulation – with therapeutic implications for aging and aging-associated diseases,” said Professor Vilchez.
Aging is a major risk factor for several neurodegenerative diseases associated with protein aggregation, including Alzheimer’s, Parkinson’s, Huntington’s and ALS. Vilchez added: “We believe that these results may be applied to other age-related neurodegenerative diseases as well as to other animal species.” A key finding was that the proteasome activity can also be increased by genetic overexpression of the activator. That way, disease-causing proteins can be eliminated even at the normal body temperature of 37 degrees Celsius. These results may provide therapeutic targets for aging and aging-associated diseases.
It has long been known that while extremely low temperatures can be harmful to organisms, a moderate reduction in body temperature can have very positive effects. For example, a lower body temperature prolongs the longevity of cold-blooded animals like worms, flies or fish, whose body temperature fluctuates with the temperature of the environment. However, the same phenomenon also applies to mammals, who maintain their body temperature within a narrow range no matter how cold or warm their environment is. For example, the nematode lives much longer if it is moved from the standard temperature of 20 degrees Celsius to a colder temperature of 15 degrees Celsius. And in mice, a slight decrease in body temperature of just 0.5 degrees significantly extends their lifespan. This supports the assumption that temperature reduction plays a central role in longevity in the animal kingdom and is a well-conserved evolutionary mechanism.
Even in humans, a correlation between body temperature and lifespan has been reported. Normal human body temperature is between 36.5 and 37 degrees Celsius. While an acute drop in body temperature below 35 degrees leads to hypothermia, human body temperature fluctuates slightly during the day and even reaches a cool 36 degrees during sleep. Interestingly, a previous study reported that human body temperature has steadily declined by 0.03 degrees Celsius per decade since the Industrial Revolution, suggesting a possible link to the progressive increase in human life expectancy over the last 160 years. (The research was conducted at the University of Cologne’s CECAD Cluster of Excellence in Aging Research.)
While overindulgence could dig you an early grave, a daily alcoholic drink may neither be harmful nor offer any health benefits, according to a new study of 4.8 million people.
The benefits and drawbacks of alcohol have been much debated. While some studies claim that even a small portion can lead to death, others say it has health benefits.
Researchers from the universities of Victoria and Portsmouth in Canada and UK respectively, conducted a systematic review and meta-analysis of 107 studies published between 1980 and 2021.
The findings showed that low and moderate drinkers have similar mortality rates to those who abstain entirely. On the other hand, women who enjoy more than one standard drink per day are at least 20 per cent likely to die prematurely.
“In this updated systematic review and meta-analysis, daily low or moderate alcohol intake was not significantly associated with all-cause mortality risk,” the researchers wrote in the paper, published on the JAMA Open Network.
However, “increased risk was evident at higher consumption levels, starting at lower levels for women than men,” they added.
The study also found no significant protective associations of occasional or low-volume drinking (moderate drinking) with all-cause mortality.
But it showed an increased risk of all-cause mortality for drinkers who drank 25 g or more and a significantly increased risk when drinking 45 g or more per day.
When they looked at previous studies that suggest people who drink a little are less likely to die early or from heart disease than people who don’t drink at all, they found the evidence was skewed by systematic bias.
“For example, light and moderate drinkers are systematically healthier than current abstainers on a range of health indicators unlikely to be associated with alcohol use, (like) dental hygiene, exercise routines, diet, weight (and) income,” they wrote. (IANS)
Dr. Ravi Kolli, President of the American Association of the Physicians of Indian Origin (AAPI), the largest ethnic medical organization in the United States was invited to be part of the 13th-anniversary celebrations of the Affordable Care Act on March 13th, 2023, at the White House in Washington, DC.
“It was such a privilege and an honor to be at the White House representing AAPI, to commemorate 13th anniversary of the Affordable Care Act. It was a memorable day to cherish,” Dr. Kolli described his experience joining with several other healthcare leaders at the White House to commemorate the Affordable Care Act signed into law by President Barack Obama. Other AAPI team members attending the White House ceremony included, Drs. Rupak Parikh, Roshan Shah, Sameer Gupta and Jay Bhat
Surrounded by several healthcare professionals, industry leaders, and heads of federal agencies, President Joe Biden along with Vice President Kamala Harris, Speaker Emerita Nancy Pelosi marked the 13th anniversary of the passage of the Affordable Care Act in the same room where his predecessor, Obama signed into law the historic Act benefitting millions.
Picture : TheUNN
The landmark Affordable Care Act also known as Obamacare was signed into law in 2010. The act aimed to provide affordable health insurance coverage for all Americans. The ACA was also designed to protect consumers from insurance company tactics that might drive up patient costs or restrict care. Millions of Americans have benefitted by receiving insurance coverage through the ACA. Many of these people were unemployed or had low-paying jobs. Some couldn’t work because of a disability or family obligations. Others could not get decent health insurance because of a preexisting medical condition, such as a chronic disease.
“Many of you joined us that day after fighting for decades to make it happen, and I remember three words I used at the time, I thought it was –” Biden said, smiling to invited guests in the White House East Room. “I thought it was a big deal. And I stand by the fact, it was a big deal.”
The president touted the progress his administration has made to advance health care policy through legislation, the Affordable Care Act. “Folks, look, we’re making health care more affordable in many other ways as well.” Biden also highlighted recent moves by several pharmaceutical companies to cap the price of insulin. “Well, I value everyone having a decent shot. It is about fairness. It is about dignity. My budget continues to build on the progress we made in the Affordable Care Act.”
Calling it historic, Dr. Kolli praised the current administration for the efforts to insure millions, providing them with affordable health benefits. Quoting statistics, Dr. Kolli pointed out, “During 2023 open enrollment a record high 16.4 million people signed up, with 4.4 million more people enrolled for health insurance since 2021. A new HHS report shows more than 40 million people are currently enrolled in Marketplace or Medicaid expansion coverage related to provisions of the Affordable Care Act — the highest total on record.”
Dr. Kolli thanked the Biden administration for the Open Enrollment outreach that was tailored to reach audiences that experience lower access to health care through cultural marketing experts to connect more people to resources including Asian American and Pacific Islander communities, African Americans, Spanish and English-speaking Latinos, and in multiple languages.
HHS released a report from the Office of the Assistant Secretary for Planning and Evaluation (ASPE) that shows more than 40 million people are currently enrolled in Marketplace or Medicaid expansion coverage related to provisions of the ACA — the highest total on record.
Referring to studies, Dr. Kolli said, ACA has helped a total of 40.2 million Americans gain coverage related based on 2022 and early 2023 enrollment data, the highest total on record. This represents 9.3 million more people enrolled than in 2021 (a 30% increase) and 27.6 million more people enrolled than in 2014 (a 219% increase, or more than triple). Survey results indicate that all 50 states and the District of Columbia have experienced substantial reductions in the uninsured rate since 2013, the last year before the implementation of the ACA.
Among the many benefits, Dr. Kolli pointed out that ACA covers many screenings and preventive services, which has been a theme advocated by AAPI: Focus on Preventive Care. “These usually have low copays or deductibles. The hope is that if you are proactive in your healthcare, you can avoid or delay major health problems later. This will benefit healthier consumers having to pay lower costs over time. For example, a diabetes screening and early treatment may help prevent costly and debilitating treatment later,” he pointed out.
Serving 1 in every 7 patients in the US, AAPI members care for millions of patients every day, while several of them have risen to hold high-flying jobs, shaping the policies and programs, and inventions that shape the landscape of healthcare in the US and around the world. For more details, please visit: www.appiusa,org
“The government is spending more in Medicare, we are getting more people with prostate cancer, more deaths with prostate cancer, [and] more metastasis with prostate cancer. While it is so simple: today, PSA is still there,” says Navin Shah, MD, MS, FACS, FICS, FACIP.
A recent study found a decrease in rates of prostate biopsy and an increase in rates of high-grade prostate cancer following a decision by the United States Preventive Services Task Force (USPSTF) to recommend against prostate-specific antigen (PSA) screening for men of all ages.1
The study retrospectively analyzed 1703 patients who underwent a prostate biopsy from 2010 to 2012 and 1006 patients who underwent a biopsy in 2018, 2019, and 2021. The 2 cohorts were stratified as Group A (having received a biopsy prior to USPSTF update on recommendations) and Group B (having received a biopsy after the USPSTF update on recommendations).
The total study cohort consisted of 76% Black patients, 14% White patients, and 11% other. Data showed that after the USPSTF recommending against screening, the annual rate of prostate biopsy went down by 41% between the 2 cohorts, from 567 patients per year in Group A compared with 335 patients per year in Group B. Despite the 41% reduction in prostate biopsies, the total number of positive biopsies doubled.
Further, the investigators found that diagnosis of high-grade prostate cancer (Gleason sum score 7-10) increased from 51.5% in Group A compared with 59% in Group B. This marked an 8% increase in high-grade disease after the recommendation was issued. They also found a 64% decrease in digital rectal examinations and a 39% decrease in PSA screening between the 2 cohorts.
In an interview with Urology Times®, Navin Shah, MD, MS, FACS, FICS, FACIP, lead author of the study, commented on these findings, saying “Screening has gone down by 50%. The digital rectal examination is down by 60%. PSA screening is down by 41%…All [that] does is increase the prostate cancer, increase the metastasis, and increase the death.”
Findings from the study are consistent with recently released data from the American Cancer Society,2 which showed that rates of prostate cancer are on the rise for the first time in 2 decades, with the leading cause of this increase attributed to the diagnosis of advanced cases of disease.
The ACS data also showed that the prostate cancer incidence rate was 70% higher among Black men compared with White men, and the prostate cancer mortality rates for Black men are 2 to 4 times higher than for other racial groups.
“We’re doing a disservice and putting harm to Black people by not screening them. What I would say that 50 years and onwards, screening should be done. Let urologists decide. Now, things are different. Now, there is active surveillance. Now, there is parametric MRI biopsy. Now, we have got [prostate-specific membrane antigen] to see whether disease has spread or not,” said Shah, who is a urologist with MidAtlantic Urology Associates in Greenbelt, Maryland.
Shah also highlighted statistics on total spending for prostate cancer by the Centers for Medicare and Medicaid Services (CMS), saying, “In 2010, when we were doing screening, [CMS spent] $10.9 billion. Then in 2016, because no screening was done, more people got metastasis, [and] the cost increased to $15.3 billion. In 2020, [CMS spent] $20 billion. So I don’t know who’s benefiting. The government is spending more in Medicare, we are getting more people with prostate cancer, more deaths with prostate cancer, [and] more metastasis with prostate cancer. While it is so simple: today, PSA is still there.”
Based on these findings, Shah and the other study authors support annual PSA screening for all men over 50 years of age, especially for high-risk patients such as Black men or those with a family history of prostate cancer. They also recommend screening for men aged 70 to 80 years, given that they found that 33% of all positive prostate biopsy patients were in that age group. Currently, the USPSTF recommends against screening for men aged 70 and older.
“You must be aggressive right from the beginning to cure the prostate cancer, not wait till it spreads and [becomes] aggressive. There is no point in that,” concluded Shah.
References
Shah N, Ioffe V, Chang JC. Increasing aggressive prostate cancer. Can J Urol. 2022;29(6):11384-11390.
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763.
Obesity is not a disease, but a lifestyle disorder that has emerged from the choices we make in terms of what we consume and how much we exercise.
It is a challenge that has been evolving rapidly in recent years and is now ranked among one of the primary causes of preventable deaths across the globe. What’s surprising is that 50 years ago, there was no disease as obesity, presumably because at the time individuals led more active lives, and did not have access to the high-calorie, processed foods that we have at present.
Decoding the primary causes of obesity
One of the primary reasons for this disorder in the current generation is the absence of physical work on a day-to-day basis, individuals have become increasingly lethargic.
Another major cause for a considerable surge in obesity rates is unorganised eating habits. There is not adequate awareness about the nutritive value of the meals we consume, and individuals usually eat without considering the effects on their health.
Today, individuals frequently consume more calories than their body requirements, resulting in weight gain and gradual obesity. However, despite the significant challenges that our current lifestyle and obesity pose to our health, they can be overcome by following these simple strategies in our day-to-day life:
Keep your calorie intake in check
To combat obesity, we must comprehend that our calorie intake should be proportional to our physical activity. This implies that we need to lead more active lives and consume meals that are nutritious and healthy. A healthy lifestyle is built on two pillars- Good nutrition and regular exercise. Disregarding either of these pillars will negatively influence our overall health.
Aim for natural weight loss
It is also essential to note that the emphasis should be on natural weight loss strategies rather than opting for cosmetic surgeries like liposuction. While these surgeries may yield temporary results, they can be detrimental in the long run. Rather, we must focus on weight loss techniques that are sustainable and healthy.
A proficient fitness coach can do wonders!
Another important element of fighting obesity is picking a fitness coach who has the required knowledge and expertise. Here, it gets crucial to understand the difference between a trainer and a teacher. While a host of individuals in the market claim to be fitness coaches, they lack the essential qualifications and experience. Hence it gets pivotal to shortlist a coach who possesses the necessary experience to advise us on the right path.
Make sustainable changes in your lifestyle
One of the most efficacious methods to fight obesity is to enlighten ourselves about the significance of healthy living. We need to be conscious of the nutritional value of the food we consume and comprehend the impact of our choices on our health.
A result-yielding strategy here would be to make short, sustainable changes in our lifestyle. For instance, we can begin by making minor changes in our diet, like lowering the intake of high-calorie, processed foods and increasing the consumption of fruits and vegetables. We can also begin by including more physical activity into our daily routine, such as walking or cycling to workplaces.
By encouraging healthy lifestyles and making healthy choices easier, we can prevent and address obesity, enhance overall health outcomes, and lessen the burden on healthcare frameworks. (IANS)
High blood pressure is typically symptomless, can quietly damage blood vessels and leads to serious health problems. While there is no cure for high blood pressure, it is important for patients to take steps that matter, such as making effective lifestyle changes and taking BP-lowering medications as prescribed by their physicians. In turn, those changes can enhance their quality of life and reduce their risk of heart and kidney disease, stroke and more.
The AMA’s What Doctors Wish Patients Knew™ series gives physicians a platform to share what they want patients to understand about today’s health care headlines, especially throughout the COVID-19 pandemic.
Here is a to-do list for patients drawn from this series on what doctors wish patients knew about addressing—and managing—high blood pressure, a condition that nearly half of adults in the United States have. Hypertension was the primary or contributing cause of death for more than 670,000 people in the country in 2020.
Many patients with high blood pressure don’t have their hypertension under control. But when patients measure their BP regularly, and share those measurements with their doctors, they are playing an important role in their care. Here is what patients need to know about taking their own blood pressure measurements outside of the clinical setting, also commonly referred to as self-measured BP.
There is a growing need for people to commit to making lifestyle changes to help prevent chronic conditions such as type 2 diabetes and heart disease, yet patients are often uncertain of what changes they should make to improve their health and well-being. This article outlines some of the key changes patients should make.
What you eat plays a leading role in your health and well-being. When someone eats healthfully, it helps to protect against many chronic diseases such as heart disease, type 2 diabetes and obesity. But with so many fad diets and food recommendations out there, it can be hard for patients to navigate what to eat and what not to eat. Two physicians offer realistic, tested advice on healthful eating.
Disrupted routines combined with the uncertainty of the pandemic have led many people to feeling isolated at home while experiencing greater stress. As a result, some people became their own bartenders and progressed into heavier drinking patterns to cope with pandemic anger, stress and anxiety. Learn when drinking is a problem, and what can be done about it.
While “lifestyle change is very beneficial for reducing blood pressure, many patients need medication to reach their BP goal,” according to Neha Sachdev, MD, a family physician who is the director of health systems relationships at the AMA. “Your doctor and you should talk about what medications are being prescribed and how the medications work to lower your BP.”
While sodium is an essential nutrient, most people consume too much and are not even aware they are doing so. Excess sodium can increase a person’s risk for developing high BP. That is why it is important to understand where most salt intake is coming from and how to lower it. Learn more about where sodium resides and which choices to make to avoid it.
High cholesterol and high blood pressure tend to run together. But, while one does not necessarily cause the other, it is common to see both in an individual. Nearly 94 million adults over the age of 20 have what could be considered borderline high cholesterol, yet as with hypertension many patients are unaware of it until they visit their doctor. Sorting through the good, the bad and the ugly about high cholesterol can be confusing. One family physician explains what to keep in mind.
The AMA has developed online tools and resources created using the latest evidence-based information to support physicians and care teams to help manage their patients’ high blood pressure.
These resources are available to all physicians and health systems as part of Target: BP™, a national initiative co-led by the AMA and American Heart Association.
Newswise — March 17 marks World Sleep Day, an annual call to action from the World Sleep Society to spread awareness of the need to get sufficient sleep to stay healthy.
Ramagopal: The amount of sleep needed varies by a person’s age. Toddlers need 11 to 14 hours daily, which includes naps. School-age children need 9 to 12 hours of sleep, teens need eight to 10 hours and adults need at least seven hours.
Ramagopal: Sleep is critical for overall good health. Lack of sleep has been shown to be associated with obesity, Type 2 diabetes, poor mental health, accidents during driving, attention or behavior problems and poor school performance.
What is good sleep hygiene?
Ramagopal: I believe the biggest factor fot people of all ages not getting sufficient sleep is because they use electronics close to bedtime. Technology stimulates your brain, which makes it more difficult to fall asleep. Even with blue light filters, the content can be a factor in preventing sleep onset.
To improve sleep, a consistent sleep schedule should be maintained, including on weekends — even though it is tempting to sleep in. Make sure the room temperature is comfortable and the room is as dark as possible. Avoid eating a large meal at least three hours before bedtime and do not consume caffeine at least six hours before going to bed. While moderate to vigorous exercise can increase sleep quality by reducing the amount of time it takes to fall asleep, you do not want to engage in vigorous activity within the hour before bedtime.
It is important for adults to model good sleep behavior for children in their home.
Is climate change affecting our sleep?
Ramagopal: New research seems to indicate that it is. A study published last year in the journal One Earth showed that increased temperature shortens sleep primarily through delayed onset, increasing the probability of insufficient sleep. The researchers estimated that by the end of the century, warmer temperatures could result in people sleeping about 8 to 10 minutes less per night.
American Association of Physicians of Indian Origin (AAPI) is excited to join in and collaborate with the over decades of service to humanity by Dr. V.K. Raju and Eye Foundation of America (EFA) to provide vision care to millions in India,” declared Dr. Naresh Parikh, President of AAPI, who has been in the forefront, identifying noble projects by Physicians of Indian Origin in India and working with them and coordinating their efforts to maximize the many services they provide across India.
AAPI has been instrumental in establishing and coordinating several projects and programs across India and established many charitable clinics, serving hundreds of thousands of people in several states in India. AAPI has been doing Global Healthcare Summit for over a decade in India and is known for its commitment to give back to India, their motherland. “The collaboration with Dr. Raju and the Foundation will help mobilize the resources at AAPI’s disposal in strengthening the efforts of Dr. Raju,” adds Dr. Parikh.
For the past four decades, Dr. Raju and the EFA have been actively and tirelessly on a crusade to eliminate avoidable blindness in areas plagued by poverty and poor access to medical care. The EFA’s mission is to eliminate avoidable blindness under the guiding principles of service, teaching, and research.
The realization of Dr. Raju’s vision, the EFA, has a reach that currently extends to 30+ developing countries and the USA. The EFA has served approximately 2.5 million patients and performed 340,000+ vision-saving surgeries, with 30,000+ surgeries performed on children alone.
The over 40 years of noble work bringing vision to millions in India started unexpectedly for Dr. Raju. While living in London, Dr. V.K. Raju traveled home to India on vacation, where a farmer asked him to examine his eyes. Dr. Raju complied, but without any instruments. In 1977, Dr. Raju returned to rural India with personnel and equipment, and offered his first eye camp near his hometown in 1977. This was the inception of the foundation’s work, beginning with the West Virginia Ophthalmology Foundation. The West Virginia Ophthalmology Foundation subsequently became the EFA in 1992.
“I feel so incredibly thankful for my personal and professional gifts, and I make great efforts to share those gifts with those in need of my services,” says Dr. Raju, and he generously gives freely of his own time, money, and medical expertise to help the less fortunate for the past several decades.
This is accomplished through eye camps and brick-and-mortar hospitals in developing countries, training of medical personnel to serve the needy, and educating the population at large on preventative eye care and healthy lifestyle choices. With adequate education, patients are empowered to take charge of their lives and their own health and prevent further deleterious consequences of their poor lifestyle choices, while sharing this knowledge with their friends and families.
The public is educated on eye care and injury prevention, and local teachers are taught how to screen for early eye problems in children. Patients, their families, and the greater community benefit from preventative medical care, free procedures, and access to education.
When education and preventative measures are insufficient, medical and surgical interventions are performed. With the aim of permanently providing world-class state-of-the art services to populations with poor access to health care, the EFA helped to build 2 hospitals in rural India: the Srikiran Eye Institute and the Goutami Eye Institute.
The Goutami Institute has a wing dedicated exclusively to children, and the EFA has future plans to build a service and research eye hospital in India where no child will be denied treatment and children from around the world can come to receive services. Dr. Raju and the EFA are also committed to finding new cures for age-old eye disease in children.
The Institute has provided service to more than 400,000 patients and 50,000 surgeries have been performed. It has become an autonomous institution, and Raju has raised over $6 million to establish and fund the two facilities. “You can never be tired of giving back,” he says. “But to have real success, your intentions should be pure. It is a spiritual act.”
Since its inception, the EFA has facilitated 600+ physician exchanges and trained 200+ ophthalmologists, equipping these medical practitioners with the tools to join the global fight against blindness. The EFA not only trains medical practitioners to join the global fight against blindness through exchange programs, but also provides workshops and training opportunities for medical students and physicians.
Born and raised in Rajahmundry, Andhra Pradesh, India, Dr. Raju earned his medical degree from Andhra University and completed an ophthalmology residency and fellowship at the Royal Eye Group of Hospitals in London, England. He is board certified in ophthalmology and is a Fellow of the Royal College of Surgeons and the American College of Surgeons. He has resided in Morgantown, WV since 1976, where he is currently a Clinical Professor of Ophthalmology at West Virginia University (WVU), the Section Chief of the Ophthalmology Department at Monongalia General Hospital, practices at Regional Eye Associates, and is the Founder and Medical Director of the EFA, a registered non-profit organization.
Dr. Raju has received many honors and awards, including 26 distinguished awards and 17 gold medals. In Dr. Raju’s adopted home state of West Virginia, he was awarded both the Lions Club International (Morgantown) Jarrett Award and the WVU International Service Award in 1995. Morgantown Rotary International presented Dr. Raju with an award for community service in 2000. He also received the Martin Luther King Jr. Achievement Award from WVU in 2008.
The American Academy of Ophthalmology (AAO) has awarded Dr. Raju 4 times for his teaching and research contributions, including the Outstanding Humanitarian Award in 2002 as Dr. Raju had donated more than $1 million dollars of his own money that went into building hospitals in India, teaching, and providing services to needy patients.
Dr. Raju received a Lifetime Achievement Award from The Association of Asian Indians in Ophthalmology in the same year and received the Free to Achieve Award from the Maryland chapter of the American Association of Physicians of Indian Origin (AAPI) for his philanthropy.
Dr. Raju’s international awards date back to the 1970s, when he received 2 separate awards for service for the blind: Lions (India) and Jaycees (Vijayawada, India). He received several gold medals, including the AP (India) Gold Medal for Contributions to Advance Ophthalmology in 2001 and the Dr. Hardia Gold Medal for Best Paper on Refractive Surgery for the All Indian Ophthalmology Society in 2002. He received the Vaidya Ratna in 2002, as well as an achievement award from the House of Lords, London, and the Mahatma Gandhi Pravasi Samman Award for Achievement in Medicine in 2014. He was also recognized as one of the Leading Physicians of the World by the International Association of Ophthalmologists in 2014. Dr. Raju was an invited guest of honor at GITAM University and the All Indian Ophthalmology Society Meeting in 2012.
Dr. Raju, who has travelled to more than 50 30 countries to help people with defective vision, says, he not only sees hundreds of patients in a day, but also teaches other eye doctors. He feels that most of his trips are enjoyable working vacations, particularly in India. “With each visit, I get my insights improved,” he says. “It is like I am getting a gift. Sometimes trips like this feel better than a holiday.”
“As I had said, the farmer I met long ago is the beginning of this work. Maybe so many friends getting involved in the Foundation’s work may be my greatest motivation,” says Dr. Raju. “Confidence is that which compels you to do the thing you think you cannot do, but you continue to do it. Many friends gave me the confidence to keep going. Many close friends were peripherally involved with the Foundation initially, but as the work of the Foundation continued, so did their involvement. This gave me incredible confidence.”
Recalling how a friend of Dr. Raju had told him that after 20+ years of foundation work, “Raju, I believed in your character. That’s why I’m very much part of it,” Dr. Raju says, “I was reminded of Abraham Lincoln’s quote, “Reputation and character are two different things. Reputation is your shadow and character is the real you.” He states, “People from distance know your reputation, but only close friends know your character. This kind of involvement from close friends maybe one of the biggest motivators for continuing the work of the Foundation.”
“Over these years, I read volumes of books by Nani Palkivala, Mortimer Adler, and some Telugu poets. This also must have motivated me. Finally, I will add this- my mother used to say, “Whatever you do, you keep on doing more and more of it.”
Doctors in America have too many comforts, he comments. “There may be some emptiness in many of us, there is also an intellectual poverty,” he says. “Some of this can be relieved by voluntary service. We have so much potential to help others — and in doing so, we may be helping ourselves much more than others.”
With all of Dr. Raju’s momentous achievements, he has also ensured that his life’s work and vision are self-sustaining. Dr. Raju has passed on his knowledge, plans, and vision to the future leaders of this movement: Dr. Leela Raju, Dr. Raju’s daughter and fellow ophthalmologist, is the EFA’s Secretary and Coordinator for Education and actively participates in its mission. Her father’s humanity and passion stimulates whatever she undertakes, Leela says. “This is not a job for him; it has never been a job,” she says. “He does his work with passion and he enjoys it. His enthusiasm and passion are infectious.”
He believes in and practices Ayurveda, an ancient Indian health care philosophy that emphasizes a holistic approach in which prevention is stressed to help lessen the need for treatment. “Eating right and exercising are the most important preventative measures according to Ayurveda,” says Dr. Raju. “The word ‘doctor’, in Latin, means teacher. A doctor’s primary responsibility is educating the patient,” he continues. In West Virginia, Dr. Raju accepts patients that do not have medical insurance and performs surgical procedures that are not covered by insurance.
India and Ghana are actively engaged in avoidable blindness elimination projects with cooperation from their governments. More than 11,560 children received vision screenings in Ghana schools; eye glasses and follow-up care were provided when necessary, Dr. Raju describes with a sense of satisfaction and pride.
Dr. Raju hopes that the AAPI joining and collaborating with successful projects such as the Eye Foundation of America’s children’s project will provide continuity of care and the mission of AAPI will be realized, benefitting millions who need eyecare.
Praising Dr. Naresh Parikh for his great vision and for seeking collaboration with several individual projects across India by numerous Physicians of Indian Origin, Dr. Raju says, “I dream to do a well-planned mega fundraiser by AAPI for a WORLD WITHOUT CHILDHOOD BLINDNESS.” According to Dr. Raju, the first project will be implemented in India. We will reach 100, 000 children in remote villages of India in the next 12 to 18 months.” Dr. Raju says, “EFA and Goutami Eye Institute have the infrastructure to accomplish this, which could be a model project.”
Dr. Raju’s charisma and vision inspire the EFA’s trainees return to their native countries to prevent and/or alleviate blindness in the field. The execution of his vision, affordable and accessible healthcare, has provided innumerable individuals with the invaluable gift of sight. In children, this gift results in 75 years of a full and productive life. These children, who would be considered a burden to society, are then able to contribute to their families and to society. Never too tired to give his best for preventing, caring, and sustaining the vision for the visually impaired, Dr. Raju says, “Our work is only just beginning.
9More than half of the world’s population will be overweight or obese by 2035 unless governments take decisive action to curb the growing epidemic of excess weight, a report has warned. About 2.6 billion people globally – 38% of the world population – are already overweight or obese. But on current trends that is expected to rise to more than 4 billion people (51%) in 12 years’ time, according to research by the World Obesity Federation.
In the 2023 World Obesity Atlas report, the organization projected that 51% of the global population will be “living with overweight and obesity within 12 years if prevention, treatment and support do not improve.”
If current trends prevail, the report also predicts childhood obesity could more than double compared to 2020 levels. “Rates are predicted to double among boys to 208 million (100% increase) and more than double among girls to 175 million (125% increase) and are rising more rapidly among children than adults,” the report states.
The World Health Organization defines overweight and obesity “as abnormal or excessive fat accumulation that presents a risk to health. A body mass index (BMI) over 25 is considered overweight, and over 30 is obese.”
Without widespread use of tactics such as taxes and limits on the promotion of unhealthy food, the number of people who are clinically obese will increase from one in seven today to one in four by 2035. If that happens, almost 2 billion people worldwide would be living with obesity. Evidence shows that obesity increases someone’s risk of cancer, heart disease and other diseases.
More than half of the world’s population could be overweight or obese by 2035, with childhood obesity predicted to more than double, a report from the World Obesity Federation has warned.
The report predicts that the economic impact of the condition could exceed $4.32 trillion per year by 2035, representing almost 3 per cent of global gross domestic product, if prevention and treatment measures are not improved.
More than half of the global population is expected to have a high body mass index (BMI) by the end of this period, with one in four people living with obesity, compared to one in seven today.
Childhood obesity rates are predicted to double among boys by 2035 and to increase by 125 per cent among girls, with lower income countries facing the most significant increases in obesity.
Nine of the 10 countries with the highest expected increases in obesity are low- or lower-middle-income countries in Africa and Asia.
The federation’s latest World Obesity Atlas annual report calls for comprehensive national action plans to be developed to prevent and treat obesity and support those affected. It also warns that without urgent and coordinated action, rates of obesity will continue to rise.
The report will be presented at a high-level policy event on March 6 to UN policymakers and member states.
While obesity is often considered a problem for higher income countries, the report reveals that obesity levels are increasing most rapidly in lower income countries, which are often the least able to respond to obesity and its consequences.
What is Obesity?
Obesity is a condition characterized by excessive body fat that can have negative effects on health. Adults are generally considered obese if they have a body mass index of 30 or above.
BMI is a value derived from the mass and height of a person. The BMI is defined as the body mass divided by the square of the body height, expressed in units of kg/m².
An adult is generally considered overweight if their BMI is between 25 and 29.9.
BMI is not a perfect measure of body fatness, as it does not take into account factors such as muscle mass or body composition. However, it is a useful tool for quickly estimating a person’s level of body fat and assessing their risk for certain health conditions.
‘Clear warning’
Prof Louise Baur, President of the World Obesity Federation, said: “This year’s Atlas is a clear warning that by failing to address obesity today, we risk serious repercussions in the future. It is particularly worrying to see obesity rates rising fastest among children and adolescents. Governments and policymakers around the world … need to look urgently at the systems and root factors that contribute to obesity, and actively involve young people in the solutions.”
Rachel Jackson Leach, Director of Science at the federation, said: “If we do not act now, we are on course to see significant increases in obesity prevalence over the next decade.”
“The greatest increases will be seen in low and lower-middle income countries, where scarce resources and lack of preparedness will create a perfect storm that will negatively impact people living with obesity the most”, she said.
In the 2023 World Obesity Atlas report, the organization projected that 51% of the global population will be “living with overweight and obesity within 12 years if prevention, treatment and support do not improve.”
If current trends prevail, the report also predicts childhood obesity could more than double compared to 2020 levels.
“Rates are predicted to double among boys to 208 million (100% increase) and more than double among girls to 175 million (125% increase) and are rising more rapidly among children than adults,” the report states.
The World Health Organization defines overweight and obesity “as abnormal or excessive fat accumulation that presents a risk to health. A body mass index (BMI) over 25 is considered overweight, and over 30 is obese.”
The increases forecast in the report would mean 1 in 4 people will be living with obesity, compared to 1 in 7 today.
“This year’s Atlas is a clear warning that by failing to address obesity today, we risk serious repercussions in the future. It is particularly worrying to see obesity rates rising fastest among children and adolescents,” said Louise Baur, president of the World Obesity Federation, in a statement about the report. “Governments and policymakers around the world need to do all they can to avoid passing health, social, and economic costs on to the younger generation. That means looking urgently at the systems and root factors that contribute to obesity, and actively involving young people in the solutions.”
While obesity is often seen as an issue for wealthier countries, where rates are generally higher, the report found lower income countries are facing rapid increases‚ adding that these countries are the “least able to respond to obesity and its consequences.”
The American Medical Association (AMA) and nearly 120 physician organizations are strongly supporting proposed reforms of prior authorization in Medicare Advantage and the Medicare prescription drug benefit.
The physician organizations sent a letter to Centers for Medicare & Medicaid Services (CMS) Administrator Chiquita Brooks-LaSure thanking her and urging the agency to finalize proposed reforms that target the inappropriate use of prior-authorization requirements by Medicare Advantage plans to delay, deny and disrupt the provision of medically necessary care to patients.
“Physicians appreciate the efforts of CMS to address the significant and multifaceted challenges that prior authorization requirements pose to Medicare beneficiaries and physicians,” said AMA President Jack Resneck Jr, MD. “We applaud CMS for listening to physicians, patients, federal inspectors, and many other stakeholders, and recognizing a vital need to rein in Medicare Advantage plans from placing excessive and unnecessary administrative obstacles between patients and evidence-based treatments.”
Among other things, CMS should finalize provisions requiring that Medicare Advantage plans:
Only use prior authorization to confirm diagnoses or other medical criteria and ensure the medical necessity of services. That is, prior authorization is not a tool to be used to delay or discourage care.
Give their beneficiaries access to the same items and services as they would under traditional Medicare. When no applicable coverage rule exists under traditional Medicare, plans must use current evidence from widely used treatment guidelines or clinical literature for internal clinical coverage criteria, which must then be made publicly available.
Establish a utilization-management committee to review their clinical coverage criteria and ensure consistency with traditional Medicare guidelines.
Not be allowed to deny care ordered by a contracted physician based on a particular provider type or setting, unless medical necessity criteria are not met.
Reforms proposed by CMS must be implemented amid mounting evidence that Medicare Advantage plans are delaying or even preventing Medicare beneficiaries from getting optimal care, resulting in alarming effects on patient health.
The most recent AMA survey found that 93% of physicians reported care delays while waiting for health insurers to authorize necessary care. Meanwhile, 82% said patients abandon treatment due to authorization struggles with health insurers, and 34% of physicians reported that prior authorization led to a serious adverse event such as hospitalization, disability—or even death—for a patient in their care.
Meanwhile, a Kaiser Family Foundation analysis found Medicare Advantage plans denied 2 million prior-authorization requests in whole or in part, representing about 6% of the 35 million requests submitted in 2021. While about 11% of denials were appealed, the vast majority—82%—of appealed denials were fully or partially overturned, raising serious concerns about the appropriateness of many of the initial denials.
“Waiting on a health plan to authorize necessary medical treatment is too often a hazard to patient health,” said Dr. Resneck. “To protect patient-centered care for the 28 million older Americans who rely on Medicare Advantage, physicians urge CMS to finalize the proposed policy changes and strengthen its prior authorization reform effort by extending its proposals to prescription drugs. We stand ready to continue our work with federal officials to remove obstacles and burdens that interfere with patient care.” (AMA)
Renowned Indian American cardiologist and cardiac electrophysiologist, Dr. Indranill Basu Ray, was awarded a Doctor of Science in Yoga by S-VYASA (Swami Vivekananda Yoga Anusandhana Samsthana), a leading institution in the field of yoga research and education.
The institute recognizes Dr. Ray’s contributions to the field of integrative medicine and his efforts to popularize the health benefits of yoga. “Dr. Basu Ray’s medical expertise has helped him develop a unique perspective on the role of yoga in healthcare,” a news release noted.
Picture : TheUNN
The prominent Indian-American cardiologist had presented a new method at the Indian Science Congress (ISC) in Bengaluru in 2020 to test the effectiveness of yoga as an intervention for treating many diseases. Indranill Basu Ray, a cardiac electrophysiologist at the Veterans Hospital in Memphis, US, presented the “new protocol” at the 107th ISC to be held from January 3-7.
“We proved tobacco was toxic not by doing clinical trials, but by following people who smoke and showing they develop a particular type of lung cancer — it would have been almost impossible to prove this using an RCT other than being phenomenally costly,” he said.
Ray claimed that “same is true for yoga, as a person who has a disease like hypertension that is due to chronic adaptation to stress may be treated with a yoga protocol to eliminate the disease.” With advanced molecular biology and commercially available wearable devices, the adaptive stress-response can be measured with yoga by monitoring hormone levels, a well-established biomarker of stress, Kolkata-born Ray said.
Every two minutes, a woman dies during pregnancy or childbirth, said a joint report prepared by multiple UN agencies.
The report, Trends in maternal mortality, reveals alarming setbacks for women’s health in recent years, as maternal deaths either increased or stagnated in nearly all regions of the world.
The sorry state
The report, which tracks maternal deaths nationally, regionally and globally from 2000 to 2020, shows there were an estimated 2,87,000 maternal deaths worldwide in 2020.
This marks only a slight decrease from 3,09,000 in 2016 when the UN’s Sustainable Development Goals (SDGs) came into effect.
Why
Roughly a third of women do not have even four of a recommended eight antenatal checks or receive essential postnatal care.
Some 270 million women lack access to modern family planning methods.
Poorest parts of the world
The poorest regions and conflict zones reported maximum maternal deaths — about 70% in sub-Saharan Africa.
Nigeria had the highest estimated number (82,000) of maternal deaths — 28.5% of all estimated global maternal deaths in 2020.
Nine countries facing severe humanitarian crises reported more than double the global maternal mortality rate — 551 maternal deaths per 1,00,000 live births, compared to 223 globally.
What about India?
India was among three countries with more than 10,000 such deaths. India reported 24,000 pregnancy or childbirth deaths, followed by The Democratic Republic of the Congo (22,000) and Ethiopia (10,000).
Where it worsened
In two of the eight UN regions — Europe and Northern America, and Latin America and the Caribbean — the maternal mortality rate increased from 2016 to 2020, by 17% and 15% respectively.
A hope
Two regions — Australia and New Zealand, and Central and Southern Asia — experienced significant declines (by 35% and 16%) in their maternal mortality rates.
Breathing is a fundamental and automatic process that sustains life. It’s a process that happens without conscious effort, but with a little bit of intention, we can use it to benefit our overall health and well-being. Breathing is the bridge between mind and body, therefore it forms the cornerstone therapy of Mind Body Medicine, a pillar of Wellness at Kshemavana.
There are several different types of breathing techniques, each with its own unique benefits. In this article, we will explore some of the most popular and widely used breathing techniques and their benefits.
Breath control is described by the Sanskrit word pranayama. It’s a technique that originated in ancient India and is widely practiced in yoga. Pranayama breathing involves controlled breathing, using specific patterns and rhythms to regulate the flow of air in and out of the body. Traditional yoga texts describe various pranayama techniques to regulate breathing. Dr. Narendra Shetty, Chief Wellness Officer of Kshemavana shares few pranayamas one can practice depending on specific needs.
Ujjayi/ Ocean’s Breath
Ocean’s Breath provides a quick way to help yourself get unstuck if you’ve been experiencing depression. Inhale through your mouth, pull in your chin so that your throat feels somewhat constricted and touches the chest, exhale while releasing the chin up, and then deliberately and mindfully inhale and exhale through your nose. At least five to ten times should be repeated.
Benefits:
It soothes the nervous system
Calms the mind and increases psychic sensitivity.
It relieves insomnia
Slows down the heart rate
Lowers blood pressure.
Although it is a calming pranayama, it also has a heating effect that encourages oxidation.
Shitali
You can use Shitali to calm yourself down when things become tense, whether emotionally or when the summer heat is at its peak. Roll your tongue in a straw-like motion. Exhale through your nose after holding the inhalation for a few seconds. Repeat.
Benefits:
Reduces excessive pitta.
Lowers body temperature and eliminates surplus heat.
Sparks the appetite and encourages healthy digestion.
Reduces excessive acidity in the gastrointestinal tract.
Relieves inflammatory skin disorders.
Assists in reducing inflammation all over the body.
Promotes mental tranquility by soothing and calming the mind.
Shitkari
You can cool down and calm your nerves by using the yogic breathing technique known as Shitkari. Roll your tongue backward where the tip of the tongue touches the inner edge of the upper palate. Breathe in through the sides of the rolled tongue and close your mouth. Exhale through your nose. Repeat.
Benefits:
Holistic Balance of the Mind and The Body.
It harmonizes the body’s Pitta (Fire Element).
Enhances Mental Health
Removes Heat from the Outside.
Promotes healthy digestion.
Fevers Treatment and Potential Cure.
Reduces high blood pressure.
Detoxifies the entire bodily system and reduces toxins.
Brahmari
If you want to unwind and let go of tension in your body, try using the humming bee breath. Simple yoga breathing techniques include taking a deep breath in through your nose and exhaling with an audible humming sound. One can close your ears with the tip of your index finger as one makes a humming sound. Feel the vibration within.
Benefits:
Reduces stress.
Improves sleep quality.
Increases mindfulness.
Reduces high blood pressure.
Improves lung function.
Enhances cognitive function
Good for Substance abuse as it reduces cravings
Bastrika
To relieve tension and stress, practice Bastrika Pranayama. It also produces a great deal of heat, which can aid in calorie burning for your body. Inhale through your nose while seated in a Lotus position. Force your breath to leave your body through your belly as if it were a “bellows” when you exhale. Do this vigorously for ten breaths, then inhale deeply, hold the breath, and exhale slowly.
Benefits:
Benefits the respiratory and digestive systems.
Drains excess phlegm from the lungs.
Improves blood oxygenation, giving all tissues and organs a boost in vitality.
Strengthens and tones the area around the abdomen.
It soothes the mind.
Energizes the entire body and mind.
Alternate Nostril Breathing
Alternate Nostril Breathing is a type of pranayama breathing technique that involves breathing through each nostril alternatively. It’s believed that this type of breathing helps balance the right and left hemispheres of the brain, resulting in a calm and centered state of mind.
Benefits:
Reduces stress and anxiety
Improves mental clarity and focus
Balances the nervous system
Increases energy and vitality
Diaphragmatic Breathing
Diaphragmatic breathing, also known as belly breathing, is a technique that focuses on deep breathing from the diaphragm, which is the muscle located at the bottom of the ribcage. In diaphragmatic breathing, the diaphragm expands and contracts, causing the lungs to fill with air, resulting in deep, slow breaths.
Benefits:
Reduces stress and anxiety
Improves sleep quality
Enhances respiratory and cardiovascular health
Boosts the immune system
Slow Breathing
Slow breathing is a technique that involves taking slow, deep breaths in through the nose and out through the mouth. It is a quick and easy method that can be used at any time and anywhere.
Benefits:
Reduces stress and anxiety
Improves respiratory function
Lowers blood pressure
Enhances mental clarity and focus
Box Breathing
Box Breathing is a simple but effective breathing technique that involves taking four equal breaths, each with a specific count. The process involves inhaling for four counts, holding the breath for four counts, exhaling for four counts, and holding the breath again for four counts. This process is repeated several times to achieve the desired level of relaxation.
Benefits:
Reduces stress and anxiety
Improves sleep quality
Enhances respiratory and cardiovascular health
Increases mental clarity and focus
4-7-8 Breathing
The 4-7-8 breathing technique is a simple and effective technique that involves counting each inhale, hold, and exhale. The process involves inhaling for four counts, holding the breath for seven counts, and exhaling for eight counts. This process is repeated several times to achieve the desired level of relaxation.
Benefits:
Reduces stress and anxiety
Improves sleep quality
Enhances respiratory and cardiovascular health
Increases mental clarity and focus
Animal Breathing
Bunny Breathing: To increase the amount of oxygen getting to your brain, take several briefs, and rapid breaths.
Bumble Bee Breathing: Slow breaths and buzzing can help reduce your heart rate and stress level.
Lion Breathing: To let out frustration and rage, take long, deep breaths and roar.
Bear Breathing: To induce a state of tranquility and restfulness, concentrate on holding your breath.
Crocodile Breathing: Deep belly breathing can be achieved by using yoga asanas like Makarasana.
Mindful breathing
If you suffer from anxiety, stress, insomnia, or high blood pressure, you might want to try mindful breathing. In order to use this technique effectively, one must fully focus their attention on their breathing. There are many different types of mindful breathing. One straightforward technique is to simply pay attention to your breath’s natural rhythm, without attempting to alter it. The breathing may naturally slow down as a result of this.
To perform mindful breathing, a person should:
find a quiet place without distractions
choose a comfortable position, ideally sitting or lying down
focus on breathing by feeling and listening to the body inhale and exhale.
Be able to let thoughts go through your mind without passing judgment.
Alternatives
Breathing techniques should never replace medical treatment. With other therapies, these exercises function best. Exercise to improve breathing may be a component of pulmonary rehabilitation for lung conditions. Exercise, physical therapy, and health information may also be a part of the treatment.
Each person will experience stress and anxiety differently. Therapy, drugs, and mindfulness practices are all potential treatment options. In stressful circumstances or to establish a regular sleep schedule, breathing exercises may help reduce stress.
Numerous medical conditions, especially stress, and anxiety, can be helped by breathing exercises. When they are a regular part of your schedule, they work best.
When people are relaxed and breathing normally, they can experiment with breathing techniques for the first time. They might benefit from practicing at the same time each day. It may take some practice to become accustomed to a breathing exercise. (IANS)
Not getting enougha sleep? It could be shortening your life, a new study suggests. According to research from the American College of Cardiology released Thursday, getting the right amount of good sleep each night can play a role in heart and overall health, which could in turn add years to your life. The data also suggests that about 8% of deaths could be attributed to poor sleep patterns.
Dr. Frank Qian, co-author of the study and clinical fellow in medicine at Harvard Medical School, told CBS News that sleep impacts many aspects of health, from hormones and metabolism to mental health and memory. From his and his team’s analysis, he was most surprised with the “potential life expectancy gain… with just fairly simple sleep quality improvements.”
The qualities they identified include:
Getting 7-8 hours of sleep a night
Having trouble falling asleep no more than twice a week
Having trouble staying asleep no more than twice a week
Not using sleep medications
Waking up feeling rested at least five days a week
While this may resemble a typical nightly routine for some, for others, especially those who rely on medication for a solid night of sleep, meeting the goals on this list could pose a challenge. According to the Centers for Disease Control and Prevention, more than a third of Americans don’t get enough sleep on a regular basis.
The study found that for those who reported meeting all five of the sleep measures listed, life expectancy was 4.7 years greater for men and 2.4 years greater for women, compared to people who met only one or none of the criteria on the list.
For those getting enough hours of sleep but still not feeling rested, Qian says it could indicate a number of things, including going to sleep distracted, sleeping in a less-than-optimal environment or having untreated sleep apnea, a sleep disorder that causes someone to intermittently stop breathing while asleep.
But he admits no one’s sleep is perfect, and that’s OK — to an extent.
“Certainly all of us… have those nights where we might be staying up late doing something or stressed out about the next day,” Qian explains. “If that’s a fairly limited number of days a week where that’s happening, it seems like that’s OK, but if it’s occurring more frequently then that’s where we run into problems.”
The research was an observational study analyzing data from 172,321 people who participated in the National Health Interview Survey between 2013 and 2018, which is fielded each year by the CDC and the National Center for Health Statistics.
More research is needed to understand the differing results between the sexes as well as what types of sleep aids or medicines are a factor and their impact.
Human brain looks years ‘older’ after just one night without sleep
Going just one night without sleep may make the brain look older, as if it had suddenly aged one to two years overnight, a new study suggests. However, these changes seem to disappear after a good night’s rest.
In the study, researchers used machine learning to generate “brain age” estimates from magnetic resonance imaging (MRI) scans of sleep-deprived people’s brains, which they compared to MRIs of those same people’s brains after a full night’s sleep. The results, published Feb. 20 in the Journal of Neuroscience (opens in new tab), suggest that one night of complete sleep deprivation produces changes in the brain similar to those seen after one or two years of aging.
Brain age is “a very interesting measure in terms of looking at how that changes from the sleep loss,” said Judith Carroll (opens in new tab), an associate professor of psychiatry and biobehavioral sciences at the University of California, Los Angeles who was not involved in the study.
The researchers pulled from five existing data sets, which included data from 134 participants in four groups: total sleep deprivation (no sleep for one night), partial sleep deprivation (three hours time in bed for one night), chronic sleep deprivation (five hours in bed each night for five nights) and a control group (eight hours in bed each night). Each group had at least one night of baseline sleep, where they spent eight hours in bed, before sleep deprivation; most groups also had a full night of recovery sleep afterwards.
Everyone had an MRI taken after each night, allowing researchers to compare how their brains looked before and after sleep deprivation, and after a full night’s rest.
The researchers determined the apparent ages of the participants’ brains using a machine-learning algorithm called brainageR, which was trained on data from more than 3,000 people. The publicly available algorithm predicts a person’s chronological age from their brain MRIs based on how healthy brains typically look at given ages, in terms of their tissue and fluid volume. In past tests, researchers found that brainageR could accurately predict age within about four years.
In their new study, the researchers found that, for the group that got no sleep for one night, brainageR estimated that they were one to two years older, on average, than they were predicted to be at baseline. These differences vanished after a night of recovery sleep.
The partial and chronic sleep deprivation groups didn’t have significant differences in their age predictions, compared to control.
These results jibe with earlier research on the effect of sleep deprivation on the brain. There’s evidence that several types of changes take place in the brains of sleep-deprived people, including changes in fluid distribution and gray matter volume.
This “widespread change in brain morphology … would be captured with this method of brain age as well,” study senior author Dr. David Elmenhorst (opens in new tab), a professor in the Institute of Neuroscience and Medicine at the research institution Forschungszentrum Jülich in Germany, told Live Science. Crucially, he framed the results not as actual aging but rather as changes that the machine-learning algorithm interpreted as aging.
Because the study found this effect only in the total sleep deprivation group, it’s hard to say what the results might mean for the effects of sleep deprivation in real life, Carroll said. “I’m not sure that we can say anything about long-term effects of chronic sleep loss, because even the chronic condition’s only five days,” she said.
The study was also relatively small. Elmenhorst said a larger sample size might highlight smaller effects in the other groups, like a brain age increase of a few months. Future research could also incorporate people who experience chronic sleep deprivation, such as people who do shift work, Carroll said.
“A lot of individuals really struggle to sleep [during the day] when they’re awake all night,” she said. “Something that looks more closely at this in those groups, I think could be really valuable and more informative.”
The global exchange of information and best practices in health would be best achieved in cooperation with doctors around the world, India’s Minister of Health said at the 13th annual conference of the Global Association of Physicians of Indian Origin (GAPIO) which took place Feb. 11-12, 2023, in Gandhinagar, Gujarat.
More than 500 doctors from 57 countries, including doctors of Indian origin practicing in the United States, the UK, and Australia among others, attended.
India’s Health Minister Mansukh Mandavia speaking at the Feb. 11-12, 2023, conference of the Global Association of Physicians of Indian Origin in Gandhinagar. Photo GAPIO
Picture : TheUNN
“The healthcare sector in India and across the world is going through transformative changes, especially after the onset of the COVID-19 pandemic,” Dr Mansukh Mandaviya, India’s Minister of Health & Family Welfare and Chemicals & Fertilizers, Government of India, said at the opening session. “Indian doctors practicing anywhere in the world have created a name for themselves. In order to further strengthen the healthcare system of the country, exchange of knowledge and information amongst doctors about global best practices is key.”
Chief Minister of Gujarat Bhupendra Patel, speaking at the Feb. 11-12, 2023, conference of GAPIO, held in Gandhinagar, Gujarat. Photo: GAPIO
Chief Minister of Gujarat Bhupendra Patel said, “While India has successfully come out of the shadows of the COVID-19 pandemic, there are greater challenges ahead in the healthcare sector due to the growing burden of non-communicable diseases such as cancer, heart diseases, and diabetes. The way forward is to provide innovative solutions which are also cost-effective and can be availed by all sections of society. Doctors have a significant role in coming up with these solutions and serving mankind.”
Founder President of GAPIO and Chairman Apollo Hospitals Group Dr. Prathap C. Reddy, said “The spirit of the physicians of Indian origin to excel in India and overseas is what we are striving to recognize. Their laudable efforts and path breaking work across the globe has made every Indian proud. The awardees’ exemplary work is an inspiration for others to emulate.”
Dr Anupam Sibal, outgoing president of GAPIO and Group Medical Director, Apollo Hospitals Group, and Senior Consultant Pediatric Gastroenterologist and Hepatologist, said, “GAPIO provides a platform to doctors of Indian origin practicing anywhere in the world to share their knowledge and exchange ideas on clinical skill development, solutions to contemporary health issues, and modernizing the approach to delivering healthcare.”
Dr Nandakumar Jairam, incoming president of GAPIO said, “Research and innovation can improve the delivery of quality healthcare in India to the last mile. As the country braces to overcome its myriad health challenges, this conference will help identify methodologies most suitable to skill and scale the healthcare workforce in the country.”
Dr. Sudhir Parikh, vice president of GAPIO speaking at the two-day conference of the organization Feb. 11-12, 2023, in Gandhinagar, Gujarat. Photo GAPIO
Dr Sudhir Parikh, vice president of GAPIO and Chairman and Publisher of Parikh World Wide Media and ITV Gold 24×7 TV Channel in United States commented, “With our presence among 57 countries, GAPIO is committed to its vision of Improving Health Worldwide. GAPIO serves to establish collaborations, bringing 1.4 million physicians of Indian origin under one umbrella platform. In the coming year, our activities will be enhanced to build a stronger well connected physician community.”
Dr. Rohini Sridhar, secretary general of GAPIO, speaking at the Feb. 11-12 conference in Gandhinagar, Gujarat. Photo: GAPIO
Dr Ramesh Mehta, past president of BAPIO (British Association of Physicians of Indian Origin) and Past President GAPIO, said, “The conference has gone beyond discussing hard-core medical specialities. Other important issues discussed such as tragedy of avoidable childhood blindness: What GAPIO can do? The evolution of Genomics: Reaching beyond the unseen, Climate change and its impact on human health, Navigating Change and Preparing for the Future – The Nursing perspective, Reversal of NCD’s, LEADS for healthcare in India, Leadership mantras, Women in Medicines make this conference really unique.”
Dr Sanku Rao, Past President, GAPIO expressed his happiness about the academic component of this conference. With around 500+ delegates, many doctors attending virtually and having more than 150 faculty members from all over the world including USA, UK, Australia and India, the conference is truly labelled as “Global” he noted.
Over two days, physicians discussed public health and the latest innovations in cardiac sciences, neurosciences, nephrology, oncology, kidney and liver transplants, gastroenterology, nutrition, and nursing among others.
A dedicated session on the use of robotics and artificial intelligence was also held. It focused on colorectal surgery, pushing the envelope by complex myomectomy with robotics, robotic upper CI surgery benefits, robotic arthroplasty, AI in cardiac disorders, artificial intelligence simplified, the role of robotics in thoracic surgery, and established and evolving indication of proton therapy in the Indian context.
During the conference, winners of the Annual GAPIO Awards to Indian physicians for noteworthy contributions to the field of medicine were also announced.
Award winners in the distinguished category:
GAPIO Lifetime Achievement Award: Prof. Dhavendra Kumar, Spire Cardiff Hospital, UK
Prathap C Reddy Philanthropy Award: Dr Rayapu Ramesh Babu, Blood Donors Organization for Social Service, Tirupati
IA Modi Award: Prof. Ajay Kumar Duseja, PGIMER, Chandigarh
GAPIO Surgical Excellence Award: Prof. Devendra Kumar Gupta, AIIMS, New Delhi
GAPIO Excellence in Diagnostic Award: Prof. Anita Borges, SL Raheja Hospital, Mumbai
GAPIO Excellence in Radiology/ Radiation Therapy Award: Prof. Akshay Kumar Saxena, PGIMER, Chandigarh
Award winners in the Young Category:
Dr IA Modi Award: Dr Sanjith Saseedharan, SL Raheja Hospital, Mumbai
GAPIO Surgical Excellence Award: Dr. Saurabh Jain, MGMMC, Indore
GAPIO Excellence in Diagnostic Award: Dr. Tushar Sehgal, AIIMS, New Delhi
GAPIO Excellence in Radiology/ Radiation Therapy Award: Dr. Chandrashekhara S H, AIIMS, New Delhi
Established in 2011, GAPIO aims to bring 1.4 million physicians of Indian origin across the world under one professional platform. Members belong to various medical specialties and super specialties, and several are recipients of distinguished awards.
Marijuana, cocaine, LSD, sedatives, opioids, heroin, and nicotine vaping—the increased use of these substances is seen to be on the rise. A continuous and addictive pattern of using dangerous substances for mood-altering objectives is known as substance abuse. The repeated usage of harmful substances without the prescription or advice of an educated person could eventually show significant health-related failures; the person could fail to meet responsibilities regarding their physical, mental, social, and emotional well-being.
Picture : Exis Recovery
The addiction to alcohol and drug intake could lead the person to develop mental health related issues and later put the individual at risk of suicidal ideations. Some immediate behavioural changes include recklessness, violence, and aggression. Long-term users may exhibit withdrawal from commitments and the public, isolation, depression, deteriorating behavior, weight loss, and decreased appetites. The following are some facts about substance abuse and suicidal ideation:
Heavy drinkers are five times more likely to die by suicide than casual social drinkers.
1 in 5 suicides involves someone who was intoxicated at the time.
Several suicides involve the use of drugs like marijuana, cocaine, or amphetamines.
According to a few studies, the frontal lobe does not fully develop until a person is in their mid-20s, which explains why young individuals have a propensity for making rash decisions on drug and alcohol intake. Other factors for the development of addiction in young adults could be associated with the curiosity that comes with age, social media toxicity, the need for adventure, experimentation, and peer pressure.
Cocaine, or the coca alkaloid obtained from the plant Erythroxylum coca, commonly known as coke or crack, acts as a neurotransmitter dopamine. It produces a stimulating effect in the human brain, which, as a result, gives out a sense of euphoria and increased energy for the users. The excessive intake of the same could cause hallucinogenic thoughts and effects in the individual. The certain effects of euphoria and a temporary feeling of happiness after the intake of the drug are what lead an individual down the road of addiction.
The first step towards prevention and control in substance abuse-related situations is to identify them. Identify, and look out for one another. Observe and communicate with the individual. The next step is to educate yourself and seek help. A number of organisations are putting in a great effort to support and help individuals struggling with addictions seek out professional and medical help. Creating awareness and providing support could also be used as measures.
Neurologists share tips for maintaining brain health throughout your lifespan
Newswise — Dementia affects millions of Americans — including nearly one in 10 adults over age 65. While the causes of different dementias vary, a 2020 report from a Lancet commission identified several modifiable risk factors that together account for around 40% of dementia worldwide.
This means that many dementia cases might be prevented or delayed by living a healthy lifestyle, said Judith Heidebrink, M.D., a neurologist at University of Michigan Health and co-leader of the Michigan Alzheimer’s Disease Research Center’s Clinical Core.
With the Lancet findings as an anchor, Heidebrink is joined by fellow neurologist and center director Henry Paulson, M.D., to share how you can reduce your risk for dementia and maintain a healthy brain throughout your life.
Keep an eye on your blood pressure
Heidebrink: Aim for a systolic blood pressure of 130 mm Hg or lower in midlife (from around age 40). Research has shown that better control of blood pressure during midlife not only reduces the risk of cognitive impairment and dementia but also of heart attack and stroke.
Protect your hearing
Paulson: Be sure to wear ear protection when you’re around excessive noise exposure to reduce your risk of hearing loss. Also, use hearing aids when needed. A recent study found that older adults who get a hearing aid for newly diagnosed hearing loss have a lower risk of dementia in the following three years.
Support efforts to reduce air pollution
Heidebrink: There is growing evidence linking air pollution, such as the gases and small particles emitted by cars and factories, to cognitive decline and dementia. Encouragingly, sustained improvements in air quality appear to reduce the risk of dementia.
Prevent head injury
Paulson: Physical damage to the brain, including traumatic brain injury, can disrupt normal brain function. Be sure to wear proper protective equipment when playing contact sports or riding a bike, wear a seat belt in cars and see a physician right away if you have concerns about a concussion or TBI.
Limit alcohol use and avoid smoking
Heidebrink: It has long been known that alcohol misuse is associated with damage to the brain and an increased risk of dementia. Limiting alcohol consumption to 1 drink per day appears safest. Smoking tobacco also increases the risk of dementia. Stopping smoking, even later in life, can help reduce the risk.
Stay cognitively engaged
Paulson: People with more years of formal education are at lower risk of dementia than those with fewer years of formal education. This is because keeping your brain cognitively engaged, helps maintain your brain health. Staying cognitively engaged can mean taking a class at a local college or online, or challenging your mind with puzzles, games or a new hobby. Socializing with others also engages your brain, so keeping up with friends and family is helpful.
Follow a heart healthy diet and maintain regular exercise throughout life
Paulson: A good rule of thumb is, “If it’s good for your heart, it’s also good for your brain.” Eating a well-rounded diet full of fruits, vegetables, and healthy fats (such as the Mediterranean diet) can help maintain a healthy weight and mitigate the risk of obesity, high blood pressure, high cholesterol and diabetes, which are known to contribute to dementia in later life.
Maintaining a regular exercise routine — 150 minutes of moderate to intense physical activity throughout your week — helps to maintain good cardiovascular health to ward off dementia.
People often forget how important simple aerobic exercise is for the brain. A brisk walk, or a stint on a stationary bike, three times a week helps your brain work better. And it’s good for your body, too.
Maintain healthy sleep patterns
Heidebrink: Sleep benefits the mind in many ways. It gives the brain a chance to lock in memories and enhances the ability to learn new skills. Current research suggests that sleep disturbances like sleep apnea may be linked to a greater risk of developing dementia. Getting enough quality sleep could help reduce your risk.
Stay socially engaged
Paulson: Studies suggest that remaining socially active throughout life may support brain health and possibly reduce the risk of dementia. Schedule regular social outings to stay socially connected with friends and family, or choose a social activity that is meaningful to you, such as volunteering or participating in community groups.
Take care of your mental health
Heidebrink: Some studies have linked a history of depression to dementia in later life. Maintaining social activities and hobbies can help ward off depression, and physical activity can help reduce stress. If you experience signs of depression, anxiety, or another mental health concern, be sure to discuss these with your health care provider.
It’s important to note that many dementia risk factors disproportionately affect minority ethnic groups.
“In addition to taking steps as individuals to decrease our own dementia risk, we should take steps as a society to ensure that everyone has equitable access to an environment and resources that promote brain health,” Heidebrink said.
For more information about dementia, including Alzheimer’s disease, Lewy body dementia, vascular dementia, frontotemporal dementia and more, visit the Michigan Alzheimer’s Disease Center website.
Many research studies are also available to contribute to our understanding of dementia, including studies that further investigate dementia in at-risk populations. If you are interested in joining a research study, please contact the Michigan Alzheimer’s Disease Center at 734-936-8332 for a full list of recruiting studies.
(Philadelphia, PA; February 8, 2023) “It is with great pleasure that we announce that the 41st Annual Convention and Scientific Sessions organized by American Association of Physicians of Indian origin (AAPI) will be held from July 6th to 9th, 2003 in the historical city of Philadelphia, PA,” Dr. Ravi Kolli, President of AAPI announced here today.
Highlighting the importance of AAPI and the contributions of AAPI members in the United states, Dr. Kolli, a senior Psychiatrist by profession said, “Today, AAPI is strong representing over 120,000 Indian American physicians, 130 local Chapters, who make up of 10% of total physicians in the US and nearly 50% of International Medical Graduates, rooted in every corner of the nation, who serve every 7th patient in the US. We are proud of our achievements and our contributions to the healthcare industry and the millions of people we serve.”
“We invite you to the 41st Annual Convention in the historic city of Philadelphia, PA,” Dr. Sanjay Gupta Convenor of AAPI Convention 2023 said. “We have convened a fantastic group of people to meet the needs of the convention and are very excited about this great event. Please reach out to any one of the representatives from the Philadelphia Host Team with questions or comments.”
Picture : TheUNN
“The 2023 AAPI Annual Convention & Scientific Assembly offers an exciting venue to interact with leading physicians, health professionals, academicians, and scientists of Indian origin,” said Dr. V. Ranga, Chair of AAPI BOT. “Physicians and healthcare professionals from across the country will convene and participate in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities in the coming year. We look forward to seeing you in Philadelphia.”
The Covid pandemic has impacted all aspects of human life as never been before. The past three years have been challenging to everyone, particularly to those who are assigned with the responsibility of caring for the sick, even as hundreds of millions are affected by the pandemic. Physicians and other health professionals on the front lines of COVID-19 care have experienced so many unknowns during the pandemic. They’ve also put their own health and the well-being of their families on the line to provide care.
“At this critical juncture in human history, AAPI, the largest ethnic medical organization in the country is focusing on themes such as how to take care of self and find satisfaction and happiness in the challenging situations they are in, while serving hundreds of patients everyday of their dedicated and noble profession,” Dr. Anjana Samadder, President-Elect of AAPI said.
Describing the importance of the host city, Dr. Satheesh Kathula, Vice President of AAPI pointed out, “Philadelphia is one of the most exciting, urban chic cities in the world. It is one of the leading regions for the Life Sciences, Energy, and Financial Services industries. Philly is home to the University of Pennsylvania and has 9 medical schools in the surrounding area will bring in many more participants and excellent world-class speakers.”
Pointing to the accessibility and convenience of reaching Philly, Dr. Meher Medavaram, Secretary of AAPI said, “Traveling to Philadelphia is only one hour and 20 minutes from New York City and 1 hour and 45 minutes from Washington, D.C. via Amtrak’s Acela Express line. Thirty airlines serve Philadelphia International Airport with 625 daily nonstop flights to 121 domestic destinations and will attract many attendees.”
Dr. Sumul Rawal, Treasurer of AAPI said, “Exhibitors and Corporate Partners will remain our top priority as we work together to provide a world-class forum for increased interactions between sponsors, exhibitors, and attendees. The ease with which attendees can move between the exhibit hall, conference and ballrooms, and their hotel rooms will ensure maximum attendance and visibility for Sponsors and Exhibitors.”
The American Association of Physicians of Indian Origin Convention offers an exciting venue to interact with leading physicians, health professionals, academicians, and scientists of Indian origin. The physicians and healthcare professionals from across the country will convene and participate in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities in the coming year.
While urging all AAPI members to make plans and be part of the historic Convention, Dr. Kolli said: “We have a wonderful team planning and organizing the event to make the 2023 annual convention a memorable experience. Please reach out to any one of the representatives from the Philly team for any of your queries.” Please visit www.aapiconvention.org for more details or call the AAPI office at (630) 990 2277 for further information.
According to a new study published in the Lancet, an estimated 6.4 million physicians are needed to meet global universal health coverage (UHC) goals. America is also experiencing a significant physician shortage, and it’s only expected to get worse, a concerning situation that could lead to poorer health outcomes for many patients. Data published in 2020 by the Association of American Medical Colleges estimates that the US could see a shortage of 54,100 to 139,000 physicians by 2033.
Europe is not in any better spot. More than three years into the pandemic that decimated personnel, healthcare managers and governments are scrambling to cobble together a semblance of a workforce in European countries. Europe’s healthcare worker shortfall—around 2 million—is acutely felt across the Continent.
In Greece, first responders sound the alarm over longer emergency response times due to a shortage of personnel. England lacks tens of thousands of nurses, reporting a record number of vacancies. Nurses top the list of all occupations experiencing shortages in Finland. Maternity wards in Portugal are struggling to stay open due to a lack of doctors. Some 50,000 healthcare workers in Europe have died due to Covid-19, and health worker absences in the European Region increased by 62% during the first wave of the pandemic in 2020, according to WHO.
The pandemic also took a severe toll on the workers’ mental health. In some countries, over 80% of nurses reported psychological distress caused by the pandemic, and 9 out of 10 nurses planned to quit their jobs.
G20, under the leadership of India and Prime Minister Narendra Modi, could offer bold solutions to this impending global healthcare crisis. While the recommendations to establish a G20 Health Preparedness Taskforce are excellent, addressing the global health workforce shortage must be a key priority in national development agendas. India can help solve the expected global physician shortage in G20 nations by investing in healthcare infrastructure and training programs. This could involve increasing funding for medical schools and postgraduate programs and improving the quality of medical education.
Additionally, India can help by expanding its role in providing medical services to underserved populations in G20 countries. This could include establishing telemedicine programs, allowing Indian doctors to provide medical care remotely. India can also work with governments in G20 nations to develop more streamlined pathways for Indian doctors to practice in those countries. Finally, India could use its public health and health systems expertise to help G20 countries develop and implement effective healthcare policies.
Here are the practical steps that G20 may take under Indian leadership:
STRENGTHEN THE MEDICAL EDUCATION FRAMEWORK
Setting up common minimum standards in the medical education of physicians, nurses, health administrators, and other allied healthcare workers among G20 nations could create a G20 medical corps that can be mobilized in the invent of emergencies due to pandemics, war, or other natural calamities. Promoting private-public partnerships and investing in new international medical schools should also be considered. We have examples of Indian universities like Manipal offering American equivalent medical education from Antigua. We also have several thousand Indian students currently completing medical education in European countries. Let G20 help execute formal agreements between G20 governments and India that define the conditions and requirements for Indian doctors to practice in those countries.
Revamping the existing guidelines for setting up medical schools and teaching methods as per future methodologies will require significant investment in e-learning tools, including remote learning, virtual classrooms, etc.
Indian medical education system is evolving and striving to reach international standards. Setting up new international medical colleges in addition to current colleges training MBBS and PG students may be considered initially. There are examples of parallel pathways in primary and secondary education in India currently offered via State syllabus in addition to ICSE or CBSE schools.
STANDARDIZING GLOBAL MEDICAL LICENSING SYSTEMS AND VISA REQUIREMENTS
Developing an online database and platform that lists the qualifications and experience of Indian doctors interested in pursuing opportunities in G20 countries would be a good start. In addition, let us work with G20 nations to create more flexible visa and work permit requirements for Indian doctors.
Furthermore, establishing a mutual recognition agreement between G20 countries and India would enable Indian doctors to practice in those countries without additional licensing exams and create standard international medical licensing guidelines. Working with G20 governments to develop and implement standardized, streamlined credentialing and licensing processes for Indian doctors and the reciprocity of national medical licenses and international clinical rotations for medical students among G20 countries should also be considered.
Facilitating and supporting the mobility of Indian doctors within the G20 countries should be promoted. We will also need to create more opportunities for G20 nations and India to collaborate on research and development initiatives.
HARNESSING TECHNOLOGY
The healthcare industry is fast-tracking the use of e-health and e-learning techniques, AI, VR simulation, and the internet of things to train, upskill and empower health workers. Telemedicine and remote patient monitoring should be encouraged among and within G20 nations involving the G20 Medical Corps, as mentioned above. The scaling-up is rapid, based on big data and analytics. These emerging technologies will also generate more demand for new skills, increasing the potential to employ more in digital healthcare delivery. Let G20 leadership help develop programs that allow G20 countries to benefit from the expertise of Indian doctors through telemedicine and other remote care services.
REBALANCING HEALTHCARE TASKS AND MANUFACTURING
As per an OECD global survey, 79% of nurses and 76% of doctors were found to be performing tasks for which they were over-qualified. Given the worldwide evidence of the poor distribution of skills, we must rationally re-organize our workforce for effective management of high-burden diseases, particularly NCDs, which are responsible for 71% of the global mortality and, unless addressed, could cost the world $30 trillion by 2030. G20 nations should also increase manufacturing and procurement of essential medical supplies domestically. Depending on China for most of your medical supplies has exposed the vulnerabilities of G20 healthcare systems during the Covid-19 Pandemic.
BRIDGING LANGUAGE BARRIER AMONG HEALTHCARE WORKERS
The newly proposed international medical and nursing students should be encouraged to be fluent in at least one or two foreign languages, which will help them bridge the language divide. For instance, several countries have similar course curriculums for nursing; however, cultural aspects sometimes need fixing. For example, Sweden and India have identical nursing curricula, and there is great potential to encourage the exchange of nurses. Still, the potential for exchange is restricted due to linguistic barriers. However, this can be easily overcome, and more conducive arrangements can be implemented to facilitate the exchange of healthcare workers.
CREATING A SUSTAINABLE AND GENDER-BALANCED WORKFORCE
Evidence points towards gender imbalance and disparities in health employment and the medical education system. According to the WHO, globally, only 30% of doctors are females, and more than 70% of nurses are females. A similar trend is seen in India, where most nursing workforce comprises women, but only 16.8% of allopathic doctors are females. As per ILO data, gender wage gaps are also a cause for concern. Therefore, we need proactive steps to create a balanced healthcare workforce that addresses the issue of gender inequity and ensures equal pay for work of equal value, a favorable working environment, and targets investments towards training the female workforce.
G20 member states under India’s leadership must increase the in-built flexibility of their health systems, showing the capacity to guarantee everyday quality healthcare for all citizens, refugees, and displaced populations. Significant investment in the future of healthcare of G20 nations is the need of this hour. The abundance of young Indian talents could help the world to minimize the expected healthcare human resource shortfall with proper training and investment. G20 countries represent two-thirds of the world’s population and four-fifths of the global gross domestic product but also a significant proportion of people left behind socially, economically, and in terms of health. Let India propose bold steps and offer solutions in healthcare to secure the future of the G20 nations.
(This story was published in The Sunday Guardian on February 11, 2023)
(Prof (Dr) Joseph M. Chalil, MD, MBA, FACHE, is an Adjunct Professor & Chair of the Complex Health Systems advisory board at Nova Southeastern University’s School of Business, Chief Strategic Officer of the American Association of Physicians of Indian Origin (AAPI), and the publisher of The Universal News Network. He recently published a best-seller book, “Beyond the Covid-19 Pandemic: Envisioning a Better World by Transforming the Future of Healthcare”.)
Heart disease is the number one Global Public Health problem. People of Indian Origin are at a four-times greater risk of heart disease than their Western counterparts and have a greater chance of having a heart attack before 50 years of age. Almost one in three in this group may die from heart disease before 65 years of age. In India, heart disease remains the number one cause of death. Nearly 36% of deaths in India are due to heart disease, and 80% of them are preventable. More than 4200 sudden cardiac arrests occur per every one lakh of the population in India annually with a survival rate of less than 10%. Immediate on-the-spot Cardiopulmonary Resuscitation (CPR) by a bystander and early use of an Automated External Defibrillator (AED) can save millions of lives across the world.
With the objective of creating awareness and providing training, especially to the First Responders, Hon’ble Chief Minister Mr. Naveen Patnaik in collaboration with Sri Sathya Sai Seva Organization, Odisha, Sri Jagannatha Service Foundation (President, Abhinav Krishna Jasthi), American Heart Association and All India Institute of Medical Sciences (Bhubaneswar) inaugurated a statewide project of Mass Hands-Only CPR training program with AED demonstration at the Kalinga Stadium in Bhubaneswar, India on February 2, 2023.
During his address, Mr. Patnaik applauded the role played by the various organizations involved with the initiative of saving precious lives. Mr. Krishna Kishore Jasthi, Principal Director of Income Tax (Investigation), Odisha, who is the chief coordinator of the project, welcomed the participants, and explained the objectives of the ground-breaking project, “Saving Lives with Bystander CPR” in Odisha.
The project was initiated by Dr. Vemuri S Murthy, an Indo-US resuscitation expert and an Adjunct Faculty in the Department of Emergency Medicine, University of Illinois College of Medicine, Chicago, Illinois. Dr. Vemuri S Murthy spoke on the importance of community CPR training and thanked the Hon’ble Chief minister for his vision and support for the statewide lifesaver project. He gave a live demonstration of Hands-only CPR and AED on a manikin for the Hon’ble Chief minister with an Indo-US AHA volunteer team of Dr. Maheshwar Parvat and Mr. Dennis McCauley.
The 9-hours long program trained nearly 2,400 participants, including 1,000 police personnel, 600 women students from R D Women’s College and Sri Sathya Sai College for Women and participants from other organizations. The plan is to train 200,000 people in the state of Odisha by the end of 2025 with a potential to save thousands of lives in Odisha. The participants received Community Bystander informational pamphlets in Oriya and “Healthy Heart” informational flyers from the American Heart Association with participation certificates.
The participants were given a brief presentation of “Heart Disease Among Women” as part of the program by Dr. Pavitra Kotini-Shah, Assistant Professor in the Department of Emergency Medicine, University of Illinois College of Medicine, Chicago, Illinois, USA. Indo-US Faculty team was honored at the conclusion of the program.
The well-organized Mass CPR program involving hundreds of volunteers was commended by the participants. Ongoing Odisha stateside programs will be planned soon, the organizers announced here.
“Efforts to raise awareness of heart disease and promoting “Healthy Heart” lifestyles is essential,” Dr. Murthy said. “Given the fact that South Asians tend to have more heart problems, it is presumed that the incidence of Sudden Cardiac Arrests might be higher in them compared to the general population in the United States. Immediate Bystander CPR (Cardiopulmonary Resuscitation) with early use of an AED can double or triple the chances of their survival. Needless to say, a concerted effort is needed to achieve the goals by all involved stakeholders, Governmental and non-Governmental, with individual participation.”
“We want to make India’s Health Care a World Class Endeavor, by utilizing: A. Information Technology; B. Field of Medicine; C. Finance, Banking; and, D. Politics. Towards this end, he recommended that the Government of India must collaborate and harness the resources available in large organizations such as the American Association of Physicians of Indian Origin (AAPI) which is the largest ethnic medical organization in the United States, representing the interests of over 100,000 Physicians of Indian origin, who serve every 7th patient, making up of nearly 15% of the healthcare professionals in their adopted country,” Dr. Sampat Shivangi, a physician, an influential Indian-American community leader, and a veteran leader of the American Association of Physicians of Indian Origin (AAPI) said, while addressing the delegates during the Pravasi Bhrataiya Diwas in Indore, India on January 9th, 2023.
As a founding member of AAPI, “I want to stress the importance of working together with solid cooperation and partnership, which will make such a tremendous change in the Indian healthcare system,” Dr. Shivangi said, while pointing out the many contributions and initiatives of AAPI and its members, who contribute immensely in several states, especially in the healthcare sector both in the urban and rural areas across India, serving millions of people.
During the recent Covid catastrophe, AAPI has provided extensive support to their motherland, he said. AAPI helped raise more than 5 million US dollars, which were used to procure and provide 2300 Oxygen Concentrators, over 100 Ventilators, 200 High Flow Oxygen, setting up dozens of Oxygen plants, and providing several Chemiluminescence Immuno-Analyzers (CLIA), each costing Rs. 50 Lakh. In addition, AAPI has adopted several villages and closely coordinated the overall development by providing primary care and preventive medicine to dozens of rural villages across India.
A conservative lifelong member of the Republican Party, Dr. Shivangi is the founding member of the Republican Indian Council and the Republican Indian National Council. Dr. Shivangi is the National President of Indian American Forum for Political Education, one of the oldest Indian American Associations. Over the past three decades, he has lobbied for several Bills in the US Congress on behalf of India through his enormous contacts with US Senators and Congressmen.
A close friend to the Bush family, he was instrumental in lobbying for the first Diwali celebration in the White House and for President George W. Bush to make his trip to India. He had accompanied President Bill Clinton during his historic visit to India.
Dr. Shivangi is a champion of women’s health and mental health whose work has been recognized nationwide. Dr. Shivangi has worked enthusiastically in promoting India Civil Nuclear Treaty and recently the US India Defense Treaty that was passed in US Congress and signed by President Obama.
Health care across the world is regarded as an important determinant in promoting the general, physical, mental, and social well-being of people around the world and can contribute to a significant part of a country’s economy, development, and industrialization when efficiently improving human health and providing access to affordable high-quality health care.
While acknowledging that India is a global leader in the manufacturing of affordable, innovative & quality pharmaceutical & medical devices across the world, realizing India’s goal of “Vasudhaiva Kutumbakam,” Dr. Shivangi pointed to how medications manufactured by Indian pharmaceutical companies “flock every shelf of American general and pharmacies, at a fraction of the cost of their American counterparts.”
Quoting studies that point to the fact that Mental Health has emerged as an “ever-challenging task,” Dr. Shivangi said, “Nearly 1 in 5 Americans has some type of Mental illness. This has caused the US government to spend $225 million in 2019 alone towards treating Mental Health. During the Covid pandemic period, 78% of adults were experiencing a mental illness, an equivalent of over 50 million Americans, with millions of adults in the USA experiencing serious thoughts of suicide, with the highest rate amongst multi-racial individuals.
Responding to realities, the US Government has initiated several measures to help people struggling with mental health issues, Dr. Shivangi said. “In the US, there are an estimated 350 individuals for one mental health provider, with programs such as Division of Prevention, Traumatic Stress, and Special Programs, Division of State and Community Systems Development, Division of Service and Systems Improvement, and National Institute of Mental Health. In addition, the Federal Government has set up several services which are easily accessible to those struggling with mental health issues, and enabling them to receive Get immediate assistance. The Veterans Crisis Line is a free confidential resource that connects veterans 24/7 with trained responders. The Disaster Distress Helpline 800- 985- 5990, which provides immediate crisis counseling to anyone facing natural or human-caused disasters,” Dr. Shivangi pointed out.
Dr. Shivangi said, they can get instant help by calling #911 in crisis; they can call or Text #988 Suicide & Crisis lifeline, a new Nationwide service, attended by trained staff, trained crisis counselors who can counsel, guide and get them admitted into nearby crisis center, community mental health center or hospital immediately that includes ambulance service. “This has caught nationwide attention. I would strongly recommend that India should think along these lines.”
The SAMHSA Substance Abuse and Mental Health Services Administration is another major initiative of the US government. I serve on the Board of SAMHSA, a prestigious position, appointed by the President of the United States. I was first appointed by President Trump & now by the current President Joe Biden.”
Dr. Shivangi praised “India for making striking progress in health standards in the post-independence era. The sustained efforts to control the country’s population & the political will to march towards the SDG in health will help India to make a significant impact in the international health sector.”
The NFHS-5 carried out in this regard during 2019-20 has shown: There were 1,020 women for 1000 men in the country in 2019-2021; TFR has also come down below the threshold at which the population is expected to replace itself from one generation to next; Child Nutrition indicators show a slight improvement at an all-India level as Stunting has declined from 38% to 36%, wasting from 21% to 19% and underweight from 36% to 32% at all India level; • Incidence of anemia in under-5 children (from 58.6 to 67%), women (53.1 to 57%) and men (22.7 to 25%) has worsened in all States of India (20%-40% incidence is considered moderate).
Full immunization drives among children aged 12-23 months have recorded a substantial improvement from 62% to 76% at all-India levels. Institutional births have increased substantially from 79% to 89% at all-India Level
Focusing on Mental Health in India, Dr. Shivangi said, “Mental Health literacy is the gateway for mental health intervention in India. However, there is a lack of awareness, which can lead to overlooking, misjudging or dismissing the signs that someone needs help.
WHO estimates 1 in every 8 individuals worldwide suffer from a mental disorder, impairment in childhood, depression, anxiety, substance abuse, & psychosis in maturity and ending with dementia in old age. 5.6 crore Indians suffer from depression, while 3.8 crore suffers from anxiety disorders. Based on the analysis, due to these factors, “India will lose 1.03 trillion in economic value” based on a study by Lancet – British Medical Journal that reported that 35% increase in mental disorders in India.
Nearly 14% of India’s population required active therapeutic interventions, while only 1 out of every 10 people gets evidence-based treatment, in other words, 70% – 80% of persons in India receive no care affiliated with it.
Pointing that there are as many as 70 million mentally ill people in the country of 1.3 billion, there are only 20,000 beds in 42 mental hospitals, due to lack of planning and funding by the government, Dr. Shivangi said. There are only 4000 qualified Psychiatrists, which is 0.2 per 100,000 population as against an average of 1.2 Psychiatrists among the nations of the world.
While the health ministry proposed to increase India’s public health expenditure to 2.5% of its gross domestic product (GDP) by 2025, it has remained within a narrow band of 1.02-1.28% of GDP. India is one of the 57 countries with a critical HRH shortage.
In inequities between the rural and urban is even more disturbing. Rural India has a shortfall of 24% Sub-Centers, 29% Primary Health Centers and 38% Community Health Centres across the country as per the Rural Health Statistics (RHS) 2020.
The national density of doctors, nurses, and midwives was found to be 20.6 per 10,000 people compared to the World Health Organization (WHO) recommendation of 44.5. There are significant urban–rural differences in HRH with urban areas having four times greater doctor density than rural areas.
Dr. Shivangi recommended that India requires 3 mental health experts for every 10,000 people, which means India needs an additional 30,000 psychiatrists, 38,000 psychiatric social workers, 37,000 psychiatric nurses.
Dr. Shivangi urged the government of India to make efforts “to educate society to provide clients with prompt mental health support, prompt intervention, cognizance, & education of the issue. Therefore it is crucial to comprehend that individuals with mental illness have a right to spend their life with dignity and self-assurance.”
Among the many suggestions, Dr. Shivangi put forth included, “Integration of mental health with primary healthcare through NMHR; Provision of tertiary care institutions for treatment of mental disorders; Eradicating stigmatization of mentally ill patients and protecting their rights through regulatory institutions like the central mental health authority & State mental health authorities; Initiate agencies on the model of SAMHSA to minimize substance abuse, a federal agency; Starting of a nationwide Tele service on the US model of 988, 911; Incentives to programs of Psychologists, Psychiatrists, and social workers in the field of mental health; and, more importantly, an awareness of mental health among the general public.”
Dr. Sampat Shivangi, an obstetrician/gynecologist, has been elected by a US state Republican Party as a full delegate to the National Convention. He is one of the top fund-raisers in Mississipi state for the Republican Party. Besides being a politician by choice, the medical practitioner is also the first Indian to be on the American Medical Association, the apex law making body.
Dr. Shivangi has actively involved in several philanthropic activities, serving with Blind foundation of MS, Diabetic, Cancer and Heart Associations of America. Dr. Shivangi has number of philanthropic work in India including Primary & middle schools, Cultural Center, IMA Centers that he opened and helped to obtains the first ever US Congressional grant to AAPI to study Diabetes Mellitus amongst Indian Americans.
Dr. Sampat Shivangi was awarded the highest civilian honor, the Pravasi Bharatiya Diwas Sanman award in 2016 in Bengaluru by the Hon. President of India, Shri Pranap Mukhejee. He was awarded the prestigious Ellis Island Medal of Honor in New York in 2008. He is married to Dr. Udaya S. Shivangi, MD, and the couple are blessed with two daughters: Priya S. Shivangi, MS (NYU); Pooja S. Shivangi who is an Attorney at Law.
Dr. Avinash Gupta, an Indian American cardiologist, has been appointed a member of the Ocean County Board of Health. The appointment took place at the regular meeting of the Board of Commissioners of Ocean County in New Jersey on Jan. 18, 2023, as per the news release.
“Gupta is looking forward to promoting public health in Ocean County,” the release stated. Specialized in Cardiology, Nuclear Cardiology, and Clinical Lipidology, he has practiced the domain for almost three decades in Lakewood, New Jersey.
Dr. Gupta is very active in community service and has served as President of the Monmouth Ocean County Association of Physicians from India (MOCAAPI) and Bihar Jharkhand Association of North America (BJANA).
Picture : TheUNN
He also holds the prestigious title of Chief of Cardiology at Monmouth Medical Center and President of the Medical Staff at Monmouth Medical Center Southern Campus.
He is chairman of Shree Siddhivinayak Temple of USA, Indian Cultural & Community Center in Toms River, and was recently elected as Executive Vice President of FIA.
Dr. Gupta was recently honored for his exemplary work in public health and social service, especially for COVID-19-related relief and humanitarian work in India and the US. “Being involved with community groups and helping others has always been my passion. Community service is very rewarding and fulfilling. It has enriched me as a person,” said Gupta who received the humanitarian award from the Monmouth Medical Center-Southern Campus Gupta at a function in New Jersey on Diwali eve.
He has been married to his wife, Dr. Geeta Gupta for over 35 years. They have one son, Abhinav who is currently in his surgical residency. Dr. Gupta has made numerous contributions to healthcare, including initiatives both in the local area and in India to promote vaccinations against COVID-19. He was recognized as an honoree at MMCSC Humanitarian Gala in October last year.
On the occasion of Republic Day, India achieved yet another milestone on the global stage as it launched the world’s first intranasal COVID-19 vaccine. Bharat Biotech’s iNCOVACC was unveiled by Dr Mansukh Mandaviya, Union Minister of Health & Family Welfare in the presence of Union Minister of State (IC) for Science and Technology, Dr Jitendra Singh, officials from the union government, co-founder and executive chairman, Bharat Biotech Dr Krishna Ella and co-founder and MD, Bharat Biotech Suchitra Ella.
World’s 1st intranasal
• iNCOVACC® is the world’s first Intranasal vaccine for COVID to receive approval for the primary 2-dose schedule, and as a heterologous booster dose, administered as nasal drops.
• iNCOVACC® is a cost effective COVID vaccine which does not require syringes, needles, alcohol wipes, bandage, etc, saving costs related to procurement, distribution, storage, and biomedical waste disposal, that is routinely required for injectable vaccines.
• iNCOVACC® utilizes a vector-based platform, which can be easily updated with emerging variants leading to large-scale production, within a few months. These rapid response timelines combined with the ability of cost-effective and easy intranasal delivery, makes it an ideal vaccine to address future infectious diseases.
• A rollout of iNCOVACC® is expected to begin in private hospitals that have placed advance orders. Initial manufacturing capacity of several million doses per annum has been established, this can be scaled up to a billion doses as required. iNCOVACC® is priced at INR 325/dose for large volume procurement by State Governments and Govt of India.
• Phase III trials (as a 2-dose regimen) were conducted for safety, immunogenicity in ~3100 subjects, in 14 trial sites across India.
• Heterologous booster dose studies were conducted for safety and immunogenicity in ~875 subjects, with BBV154 intranasal vaccine administered in those previously completing a regimen of the commonly administered COVID vaccines. The trials were conducted in 9 trial sites across India.
• iNCOVACC® recipients demonstrated significant levels of Mucosal IgA antibody levels (measured in the saliva). Mucosal IgA antibodies in the upper respiratory tract may provide benefits in reducing infections and transmission. New Delhi/Hyderabad, Jan 26, 2023: Bharat Biotech International Limited (BBIL), a global leader in vaccine innovation and developer of vaccines for infectious diseases, today dedicated iNCOVACC® (BBV154) to the nation, world’s 1st COVID intranasal vaccine for Primary series and Heterologous booster.
Picture : TheUNN
iNCOVACC® was launched by Dr. Mansukh Mandaviya, Hon’ble Minister for Health and Family Welfare, in the presence of Dr. Jitendra Singh, Hon’ble Minister for Science & Technology, on the occasion of Republic Day. Product development and clinical trials for iNCOVACC® were funded in part by the Government of India, through the Department of Biotechnology’s, COVID Suraksha Program.
Bharat Biotech received approval from the Central Drugs Standard Control Organization (CDSCO) for iNCOVACC® to be administered for primary series and as heterologous booster doses.
Amid growing COVID- 19 cases and emerging variants of the highly transmissible virus, a booster dose of the vaccine becomes imperative. iNCOVACC® is now available on CoWIN, and priced at INR 800 for private markets and INR 325 for supplies to Govt of India and State Governments.
iNCOVACC® is a recombinant replication-deficient adenovirus vectored vaccine with a pre-fusion stabilized spike protein. This vaccine candidate was evaluated in phase I, II and III clinical trials with successful results.
This vaccine has been specifically formulated to allow intranasal delivery through nasal drops. The nasal delivery system has been designed and developed to be cost-effective in low and middle-income countries. As a needleless vaccination, Bharat Biotech’s iNCOVACC® will be the world’s first such booster dose. India will now have more options when it comes to third doses or precautionary doses.
Clinical trials and extensive humoral and cell mediated responses were conducted to evaluate iNCOVACC® as a primary dose schedule, and as heterologous booster dose for subjects who have previously received two doses of the two commonly administered COVID-19 vaccines in India. The intranasal vaccine is stable at 2- 8°C for easy storage and distribution and has been designed for efficient distribution and easy pain free administration.
iNCOVACC® was developed in partnership with Washington University, St. Louis, which had designed and developed the recombinant adenoviral vectored construct and evaluated in preclinical studies for efficacy.
The number of people dying from cardiovascular disease (CVD) in the US escalated during the first year of the Covid-19 pandemic, from 874,613 CVD-related deaths recorded in 2019 to 928,741 in 2020, a new study has revealed.
The rise in the number of CVD deaths in 2020 represents the largest single-year increase since 2015 and topped the previous high of 910,000 recorded in 2003, according to the data published in American Heart Association’s flagship, peer-reviewed journal Circulation.
It means that more people died from cardiovascular-related causes in 2020, the first year of the pandemic, than in any year since 2003, according to data reported in Association’s 2023 Statistical Update. The largest increases in deaths were seen among Asian, Black and Hispanic people.
“While the total number of CVD-related deaths increased from 2019 to 2020, what may be even more telling is that our age-adjusted mortality rate increased for the first time in many years and by a fairly substantial 4.6 per cent,” said Connie W. Tsao, assistant professor of medicine at Harvard Medical School.
“I think that is very indicative of what has been going on within our country, and the world, in light of people of all ages being impacted by the Covid-19 pandemic, especially before vaccines were available to slow the spread,” said Tsao, also an attending staff cardiologist at Beth Israel Deaconess Medical Center in Boston.
There was a substantial increase in the loss of lives from all causes since the start of the pandemic. “That this likely translated to an increase in overall cardiovascular deaths, while disheartening, is not surprising. In fact, the Association predicted this trend, which is now official,” said Michelle A. Albert, the American Heart Association’s volunteer president and a professor of medicine at the University of California at San Francisco (UCSF).
The virus is associated with new clotting and inflammation.
Several people who had new or existing heart disease and stroke symptoms were reluctant to seek medical care, particularly in the early days of the pandemic.
“This resulted in people presenting with more advanced stages of cardiovascular conditions and needing more acute or urgent treatment for what may have been manageable chronic conditions. And, sadly, appears to have cost many their lives,” said Albert.
Cardiovascular disease continues to be the top killer globally, taking the lives of more than 19 million people around the world each year, including people of all ages, genders and nationalities.
“Sharing of knowledge and best practice has been a key component of AAPI’s Global Healthcare Summit,” Dr. Ravi Kolli, President of the American Association of Physicians of Indian Origin (AAPI), while describing the objectives of the recently concluded Global Healthcare Summit, said here.
Attended by nearly 500 delegates from the United States and India, the GHS 2023 was jointly organized by AAPI and the local organizing committee at Visakhapatnam from January 6th to 8th, 2023. This Global Health Care Summit, with participation from leading medical professionals, thought leaders, heads of several health industry sectors, and policy-makers has had a vibrant and most enriching series of educational seminars and workshops.
“The essence of AAPI is educational,” Dr. Kolli added. “That translates into numerous Continuing Medical Education (CME) and non-CME seminars by experts in their fields. The GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” has had several CME sessions that focused on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, research, and Medical Jeopardy.”
CME sessions with academicians from the United States offered unique opportunities for local medical staff and healthcare professionals to advance their learnings and provide the best possible care for the people of India. The Summit had a research competition for medical students and postgraduate students from all over India. AAPI conferred Awards of excellence and lifetime achievements during the Summit.
A major theme of the GHS 2023 was Metal Health. The much-anticipated CME on Psychiatry coordinated by Dr. Rao Mowwa began with an excellent presentation on “State of Psychiatry and Psychiatric Training in India” by Dr. N. N. Raju on Friday, January 6th. The session on “Prevention of suicide through safety planning – a proactive approach” by Dr. Bush Kavuru, and on “Creativity and Insanity: Two Sides of Same Coin?” by Dr. Indla Ramasubbareddy educated the audience on ways to understand and appreciate mental health issues in individuals and offer support, which will help them live a productive and dignified life. Dr. Ravi Koll provided an overview of the need for gratitude and appreciate the blessings in life through an insightful session on “Science and Practice of Gratitude in Wellbeing.” Dr. Srinivas Gokarakonda and Dr. Vijay Maurya moderated the sessions.
The second part of the morning session was on Diabetes and Kidney Disease. The scientific presentation on Diabetes Management Update was given by Dr. G.R. Sridhar, while “Diabetic Nephropathy: Current Concepts in Diagnosis” was offered by Dr. Sharma Prabhakar. Dr. K. L. Gupta educated the audience on Lupus Nephritis. “CKD of Unknown Origin & Uddanam Nephropathy” was the theme addressed by Dr. T. Ravi Raju, while “New Insights into the Biology and Mechanism of Renal Fibrosis” was the topic addressed by Dr. Raghu Kalluri. The sessions were moderated by Dr. KAV Subrahmanyam, Dr. K. Dilip Kumar, and Dr. R. K. Sharma.
The first-ever “JAAPI Symposium on Development of Non-Communicable Diseases in India” was moderated by Dr. Suresh Karne. Non-Communicable Diseases (NCDs): A Global Health Challenge in the 21st Century was the theme addressed by Dr. Soumya Swaminathan, a former Chief Scientist at World Health Organization. Dr. Suzanne Tanya Nethan provided an overview on “Non-Communicable Disease Risk Factors and Their Trends in India” while a presentation on “Intergenerational Transmission of NCDs in Developing Countries and in India” was given by Dr. Chittaranjan Yajnik. The Role of Infant Nutrition in the Development of Adult Onset of NCDs was addressed by Dr. Ramasubbareddy Dhanireddy.
The AAPI delegates were led to a Meditation Session by Mrs. Sheerisha on Saturday morning. Apollo Session of Cardiology on Saturday was led by Dr. Sreeni Gangasani, AAPI’s CME Chair, and was moderated by Dr. D. K. Baruah, Dr. C. Ravi Venkatachelam, and Dr. Sujeeth Punnam.
N K Panigrahi opened the session with a brilliant talk on Heart Disease Epidemic, which was followed by an informative session on Heart Failure- What’s New for 2022, presented by Dr. Sreeni Gangasani. Dr. A. Sharath Reddy spoke on Interventional Cardiology Update, and Dr. Brahma Sharma educated the delegates on Current Concepts in Prediction and Prevention of Heart Attacks in South Asians. Structural Heart Disease was the theme of the presentation by Dr. Prasad Chalasani, while Update on Cardiac Surgery was presented by Dr. M. Gopichand.
The Biophore Session on Gastroenterology was moderated by Dr. G. Santarao and Dr. SNR Naveen. Dr. Nagendra Myneni updated the delegates on Hepatitis, while Lap GI Surgery Update was given by Dr. C. Palanivelu. Hepatocellular Carcinoma was the topic addressed by Dr. Sudhakar Jonnalagadda, and “An Integrative Medical Approach to Common Gastroenterological Conditions” was the theme discussed by Dr. Vijaya Voruganti.
The session on LVPEI Blindness Prevention was moderated by Dr. C. V. Gopala Raju and Dr. P Viswamithra. Dr. Gullapalli N. Rao gave an overview of Global Blindness Statistics & Vision 2020 Outcomes, while Global Glaucoma Blindness – Magnitude & Management was the topic addressed by Dr. Sriram Sonty. Blindness in South East Asia – Prevention Strategies was the focus of the address by Dr. Rohit Khanna, while Childhood Blindness was the theme by Dr. V. K. Raju. Dr. Harsha Bhattacharjee shared insights from a case study on Blindness Relief Program in Northeast India.
NATCO Pharma Oncology Session on Sunday, January 8th was chaired by Dr. Satheesh Kathula, Vice President of AAPI, and moderated by Dr. Muralikrishna Voonna and Dr. Sushil Jain. “A focus on newer treatment modalities in Radiation Oncology” was the topic addressed by Dr. Umesh Mahantshetty, while Dr. T. Subramanyeswar Rao spoke about “What’s new in surgical oncology?” An Update on Systemic Therapies for Cancer was provided by Dr. Raghunadharao Digumarti. “Evolving Biology and New Therapies – Strategies to Control Cancer” was the topic addressed by Dr. Raghu Kalluri. An insightful session on Pharmaco economics of cancer drugs – can we afford it?” was presented by Dr. Satheesh Kathula. “India’s unique value proposition towards Medical Tourism” was addressed by Mr. Shaaz Mehmood.
The session on Infant Mortality: Current Trends was led by Dr. Raja Nandyal and Dr. Sashi Kuppala. The session on Neurology had Dr. Suresh A. Reddy as the lead speaker, who spoke on “Stroke and Interventions,” while Acute stroke and post-stroke management in India was the topic addressed by Dr. K. Venkateswarlu. Head Injury Management was the topic discussed by Dr. Krishan Kumar, and Challenges and Opportunities in providing Epilepsy care in India was the topic addressed by Dr. Malla Bhaskara Rao. Neonatal Resuscitation sessions were led by Dr. Raja Nandyal and Dr. Sumitra Reddy. Education on Neuro Emergency – ENLS was provided by Dr. Leena Gupta.
Prem Reddy Foundation Medical Jeopardy was brilliantly coordinated by Dr. Harsha Thirunagari, Dr. A. P. Naveen Kumar, and Dr. P Venu Gopal, while the Advisor was Dr. Leena Gupta. Poster Presentations provided an opportunity for aspiring young physician students to showcase their research and knowledge in addressing healthcare needs across the nation. The contest was judged by Dr. A. Bhagyalakshmi, Dr. A. Mythili, Dr. Sharma Prabhakar, and Dr. Raghu Kalluri.
The much-anticipated Women’s Leadership Forum featured extraordinarily successful Women Leaders representing a diversity of professions, involving public, private and government organizations.
Dr. Smt. Tamilisai Soundararajan Honorable Governor of Telangana & Lt. Governor of Puducherry delivered the keynote address at the Women’s Forum, chaired by Dr. Udaya Shivangi and Dr. T. Radha, while Dr. Uma Jonnalagadda is the Advisor and Dr. B. Devi Madhavi is serving as the Co-Chair. According to Dr. Shivangi, “The eminent speakers at the Women’s Form deliberated on ways to: Advancing Women’s Health Through Awareness and Action.” Shri. MVV Satyanarayana, Member of Parliament, representing Visakhapatnam was the Guest of Honor at the Women’s Forum, while Dr. Udaya Shivangi, Dr. T. Radha, Dr. Uma Jonnalagadda, Dr. B. Devi Madhavi, and Dr. Ramani moderated the session.
The Summit featured a CEO Forum, where a galaxy of CEOs from around the world from hospitals, teaching institutions and major healthcare sectors, including pharmaceutical, medical devices and technology, shared their expertise and explored potential opportunities for collaboration. Shri. Biswa Bhusan Harichandan, Honorable Governor of Andhra Pradesh will be the keynote speaker at the CEO Forum 2023 with the theme, focusing on “True and Total Health is the well-being of the Mind, Body, and Spirit for holistic person-centered care.” Dr. Ravi Kolli, AAPI President led the discussions, while Prof. MD Nalapat served as the Co-chair along with Prof. Joseph M. Chalil, MD, Co-chair & AAPI Chief Strategy Officer. “We envision a great future for our country with the direct result of complex interactions at this forum with your assistance, guidance, and experience,” Dr. Chalil said.
Medical Education & Research was led by Dr. Lokesh Eadara, Dr. P.V. Sudhakar, and Dr. G. Butchiraju. Community Outreach Program – HPV Vaccination at the Mahatma Gandhi Cancer Hospital, Visakhapatnam was coordinated by Dr. Syed Ahmed, Dr. Murali Krishna Voona, Dr. Meher Bala Medavaram, Secretary of AAPI.
The 16th annual Global Healthcare Summit (GHS) organized by the American Association of Physicians of Indian Origin (AAPI) came to a close with a call and commitment to give back to India, our motherland, helping healthcare accessible, efficient and equitable for all at Hotel Novotel on the seashore in Visakhapatnam on January 8th, 2023.
“In our quest to fulfill the mission of AAPI, we are proud to share best practices and experiences from leading experts in the world and develop actionable plans and projects that enable access to affordable and quality healthcare for all people. To help accomplish this mission, we are excited to be here in Visakhapatnam and lead the GHS 2023,” Dr. Kolli said. For more information, please visit: www.aapiusa.org
The 16th annual Global Healthcare Summit (GHS) organized by the American Association of Physicians of Indian Origin (AAPI) concluded with a call and commitment to give back to India, our motherland, making healthcare accessible, efficient, and equitable for all, at Hotel Novotel on Varun Beach in Visakhapatnam on January 8th, 2023.
Attended by nearly 500 delegates from the United States and India, the GHS 2023 was jointly organized by AAPI and the local organizing committee at Visakhapatnam from January 6th to 8th, 2023. This Global Health Care Summit, with participation from leading medical professionals, thought leaders, heads of several health industry sectors, and policy-makers has had several unique events with enthusiastic participation from local healthcare fraternity and dozens of leading physicians from the United States.
Dr Ravi Kolli, President of AAPI, while describing the objectives of the Summit, said, “The Global Healthcare Summit has served as a means to raising awareness on key health care issues affecting the Indian subcontinent, such as the Stigma of Mental illness, Suicide prevention, Diabetes, Cardiovascular Diseases, Women’s and Children’s Health, Blindness Prevention and Hepatitis etc. Highlight of this Summit was to reaffirm NRI Physicians’ commitment towards improving health care and create model programs for management of various diseases and to improve outcomes universally, he added.
The Summit focused on mental health, including reducing the stigma for seeking mental health services, and on Physicians burnout, Dr. V. Ranga, Chair of AAPI BOT said. “Deliberations included discussions on the Stigma of Mental illness, Suicide prevention, Management of Chronic and Non Communicable Diseases, and other Global Health issues including Climate Change and its impact on population health,” he added.
In addition, AAPI has plans to collaborate with various state and federal government programs to enhance the quality of healthcare delivery, making it affordable, efficient, and equitable, improving health outcomes universally and training the trainer sessions involving learning modules in different specialties, and tele-consultations.
Shri. YS Jagan Mohan Reddy, Honorable Chief Minister of Andhra Pradesh, in a message delivered to the AAPI delegates at the GHS, urged the members of “the American Association of Physicians of Indian origin to give back something to the society, which has given them an opportunity to pursue medical education and become successful in India and abroad.” He expressed confidence, stating, “I’m sure this platform will bring together best in the healthcare field from professionals, who will provide innovative solutions for the challenges being faced by all.”
Chief Guest at the Summit, Smt. Vidadala Rajini, Honorable Minister for Health, Family Welfare & Medical Education of state of Andhra Pradesh, said, “The Global Healthcare Summit is an important opportunity for all the healthcare professionals to learn from each other and enhance fellowship. I’m grateful to have this opportunity to attend and learn from all of you,” she said. “I believe that by working with you, we can improve the health and wellbeing of the people in the state. The government has the ability to design the best policies on healthcare, while delivering the best treatments and medical care to the patient is essentially in the hands of the physicians.” Among others who addressed the AAPI delegates and joined the felicitation of AAPI delegates and the local organizers of the Summit included, Shri. Gudivada Amarnath, Honorable Minister for IT.
“We are sure that the Summit offered a rewarding experience not only on intellectual but on aesthetic front as well, with the scenic beauty of Visakhapatnam and the many surrounding places. The organizing committee has taken every measure possible to make the event a memorable one for everyone at the GHS,” said Dr. Ravi Raju, Chair of GHS (India) 2023.
Describing some of the objectives of the GHS, Dr. Prasad Chalasani, Chair of GHS (USA) 2023 said. “We have tried to create an intellectually charged platform for experts to share their knowledge and experiences on some of the common professional issues that remain a challenge in spite of all the advances. The exchange of expertise and transfer of technology by the best brains is bound to offer positive and innovative solutions to some of the problems faced by humankind.”
Among the many initiatives that emerged from GHS 2023, a notable action plan has been for AAPI to collaborate with the Government of Andhra Pradesh to initiate an ambitious program to address mental health and wellness of students in high school in Andhra Pradesh. Some of the other initiatives that were announced during the GHS 2023 included: effective treatment modalities on non-communicable medical diseases, reducing the infant and maternal mortality and HPV Vaccination.
The essence of AAPI is educational. That translates into numerous Continuing Medical Education and non-CME seminars by experts in their fields. The GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” has had several CME sessions that focused on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, Spiritual presentations and Medical Jeopardy for Medical students.
CME sessions with academicians from the United States offered unique opportunities for local medical staff and healthcare professionals to advance leanings and provide the best possible care for the people of India. The Summit had a research competition for medical students and post graduate students from all over India. AAPI conferred Awards of excellence and lifetime achievements during the Summit.
AAPI, in collaboration with the AAPI India Foundation administered free HPV vaccines to over 100 low income young women from several government schools in the region, during a special launch and awareness camp organized at the Mahatma Gandhi Cancer Hospital, Visakhapatnam in India on Saturday, January 7th, 2023 with the objective of creating awareness and preventing cervical cancer, a leading cause of cancer deaths among women in India.
“We at AAPI, in keeping with our efforts and initiatives to educate, create awareness and provide support on disease prevention, are happy to be part of the HPV Vaccine Awareness Program,” Dr. Ravi Kolli, President of AAPI said. “It was truly an enriching experience to be present in person and meeting with the young women and be part of this life saving mission.”
“Advancing Women’s Health Through Awareness and Action” was the theme at the much-anticipated Women’s Leadership Forum that featured extraordinarily successful Women Leaders representing a diversity of professions, involving public, private and government organizations. Panelists at the Women’s Forum included: Dr. Suneela Garg, Dir. Professor & Head of Community Medicine at Maulana Azad Medical College; Dr. Anuradha Medoju, Senior Regional Director at Telangana & Andhra Pradesh Ministry of Health & Family Welfare, Government of India; Dr. S. Radha Rani, Former Professor and Superintendent, Hospital of Mental Health; and Ms. Meghna Chalasani, Team Lead, Advisory Committees, Program Lead, Science Office Strategies for New Drugs at Center for Drug Education and Research, US Food & Drug Administration.
Dr. Smt. Tamilisai Soundararajan Honorable Governor of Telangana & Honorable Lt. Governor of Puducherry delivered the keynote address at the Women’s Forum virtually. She urged everyone to “Pay attention to little things and how changes can be brought in. Services need to reach everyone. There are many plans and programs initiated by the government, but people need to be made aware of them and be helped to utilize the programs,” she said. She lauded “the great work by AAPI members for promoting health globally.”
Dr. Udaya Shivangi, Chair of AAPI’s Women’s Committee, in her opening remarks provided an overview of the Forum and the many initiatives by the Forum both in India and the United States. Shri. MVV Satyavathi, Member of Parliament, representing Anakapalli was the Guest of Honor at the Women’s Forum. In her address, she congratulated AAPI, whose members having been born and educated in India, settled down in the US with success, have come back to India to serve the people of India and work together for the betterment of humanity.
The Summit featured a CEO Forum, where a galaxy of CEOs from around the world from hospitals, teaching institutions and major healthcare sectors, including pharmaceutical, medical devices and technology, joined to explore potential opportunities for collaboration.
Shri. Biswa Bhusan Harichandan, Honorable Governor of Andhra Pradesh was the keynote speaker at the CEO Forum 2023 with the theme, focusing on “True and Total Health is the Well-being of the Mind, Body, and Spirit for holistic person-centered care.” Dr. Ravi Kolli, AAPI President led the discussions, while Prof. MD Nalapat served as the Co-chair along with Prof. Joseph M. Chalil, MD, Co-chair & AAPI Chief Strategy Officer. “We envision a great future for our country with the direct result of complex interactions at this forum with your assistance, guidance, and experience,” Dr. Chalil said.
A galaxy of speakers who were part of the powerful CEO Forum included: Ambassador Pradeep K. Kapur; Dr. Sangita Reddy. a Global Healthcare Leader, Indian Entrepreneur, and Humanitarian; Dr. Juby A Jacob-Nara, Vice President, Head of Global Medical- Respiratory Allergy & Gastroenterology (Sanofi-Genzyme), Mr. Sadasiva Rao Nannapaneni, Vice President – Corporate Affairs, Legal & Secretarial, Estate Management at NATCO; Dr. Anu Chirala, Co-Founder & President InstaMD; Dr. Jagadeesh Babu Rangisetty, CEO at Biophore India Pharmaceuticals Pvt. Ltd, who has more than 30 years of experience in the Pharmaceutical Profession; Mr. Ramprasad M, Chairman, SHAI and an Investment banker, Dr. Upendra Srinivas, Managing Director at Quantum Specialty Diagnostics; Dr. Venkat Ramana Sudigali, Founder-Director Excell Multispecialty Hospital, Hyderabad, India, and the CEO of EHA Consortium.org; and Mr. Sasi Sunkara, Executive Director and Co-founder at CIPHER Oncology
Dr. Soumya Swaminathan, former World Health Organization (WHO) chief scientist was conferred with the prestigious Prof P. Brahmayya Sastry Oration & Dr. T. Ravi Raju Excellence Award during the Summit in Visakhapatnam on Friday, January 6, 2023. The event jointly organized by Prof P. Brahmayya Sastry Memorial Oration Committee and Andhra Medical College, Visakhapatnam was chaired by Dr. Abhijat Sheth and Dr. Sridhar Chilimuri.
The women leaders of AAPI dazzled on stage with elegance, and showcasing their talents by presenting two amazing Fashion Shows on Friday and Saturday at the Summit to the delight of the AAPI delegates.
Led by Surgeon Rear Admiral R. Ravi, Command Medical Officer, Eastern Naval Command, Visakhapatnam, nearly 500 students from local schools and colleges, and dozens of delegates at the 16th annual Global Healthcare Summit participated at the Walkathon on the serene oceanside of the Bay of Bengal at Visakhapatnam on a beautiful Sunday morning on January 8th, 2023 with a mission to create awareness on Mental Health with the theme: “Be the Change: All for Global Health.”
In his closing remarks, Dr. Ravi Kolli said, “The Global Healthcare Summit held annually in India across several states, has become a major contributing factor, where Indian American Doctors focus on various programs and policies in our efforts to make a huge difference in the delivery of healthcare in India.”
“After the highly successful Global Healthcare Summit in Visakhapatnam last weekend, I am happy to announce that the 17th annual Global Healthcare Summit will be held in New Delhi from January 2nd to 4th, 2024,” Dr. Anjana Samadder, President-Elect of the American Association of Physicians of Indian Origin (AAPI) announced here during a Curtain Raiser held at the prestigious Constitution Club in New Delhi on January 9th, 2023.
“In our quest to fulfill the mission of AAPI, we are proud to share best practices and experiences from leading experts in the world and develop actionable plans and projects that enable access to affordable and quality healthcare for all people. To help accomplish this mission, we are excited to be here in Visakhapatnam and be part of the GHS 2023,” Dr. Kolli urged. For more information on Global Health Summit, please visit: www.summit.aapiusa.org and www.GHS2023.com
Tyson Center in Floral Park, New York witnessed the colorful installation of the incoming governing board of Indian Nurses Association of New York (INANY) for the term 2023-24 in the presence of members of INANY, their families, community leaders and elected Indian American officials.
The executive board and the advisory board lighted the lamp and received Proclamation from Senator Keven Thomas, the only Indian American Senator in New York State senate.
Picture : TheUNN
Dr. Anna George (president), Dr. Shyla Roshin (vice president), Alphi Sundroop (secretary), Dr. Jessy Kurian (joint secretary), Jaya Thomas (treasurer), and Aleyamma Appukuttan (joint secretary) constitute the executive board. Tara Shajan (chair), Mary Philip, Usha George, Sosamma Andrews, and Honorable Dr. Aney Paul will continue as the advisory board. The chairs of various committees are Dr. Solymole Kuruvilla (bylaws), Salil Panakal (Awards and Scholarships), Anto Paul (education and professional development), Mary Philip (election), Sini Varghese (advanced practice nurse forum), Paul Panakal (communications), Jessy James (cultural and social programs), Shabnampreet Kaur (membership), Annie Sabu (fundraising and charity), Dr. Ani Jacob (research and grants). Esthor Devadoss, Grace Alexander, Lyssy Alex and Aleyamma Mathew will be area coordinators. Mary Philip and Paul Panakal organized and smoothened the ceremonial process followed by Mary Philip’s administration of the oath.
The only Asian elected to New York State senate from district 6 in Long Island was eloquent of his own familiarity with the activities that INANY serves. He expressed his gratitude of what INANY did for outreach to the underserved individuals and families in his constituency by organizing and conducting health fair and blood drive for the community. He promised that he would continue to advocate for the nurses who he said, are the people working very hard in hospitals and nursing homes. Tara Shajan, the chair of the advisory board introduced and welcomes the senator.
Picture : TheUNN
The reelected president Dr. Anna George was introduced and welcomes by her student Shabnampreet Kaur. Dr. George showcased the contributions of INANY to the educational and professional development of nurses, for the mental health of nursing after the pandemic, involvement of the Association in the health of communities in need and the efforts to mitigate the surge of anti-Asian hate incidents since the beginning of COVID-19.
Suja Thomas, the incoming president of National Association of Indian Nurses of America was a keynote speaker. She was introduced by Anto Paul. Suja expressed her gratitude for INANY’s professional and social initiatives for health and healthcare both within and outside of the communities. She, as the leader of the national association, offered and requested support.
Honorable Dr. Aney Paul who took the lead in forming INANY and was the founding president, continues to serve in its advisory board. As the first Indian nurse ever elected in the United States as a legislator, she always stood for the welfare of nurses and also initiated health related legislations in her county of Rockland. She currently serves as the vice chair of Rockland County legislature. She talked about how gratified and happy she was being part of INANY and being experiencing the good things INANY does for both nurses and the society at large.
Picture : TheUNN
Honorable Ragini Srivastava, the recently elected Town Clerk of North Hempstead was introduced by INANY’s outgoing vice president Dr. Solymole Kuruvilla. Ms. Srivastava who immigrated to the US from India became a successful business woman and rose to become the first Indian American Town Clerk in Long Island. Ms. Srivastava spoke highly of INANY and the leadership’s concern for the poor and the underserved community. She praised and thanked the constantly compassionate and empathetic care the Indian nurses in the area provide thousands and thousands of persons and their resiliency they evidenced especially during the pandemic.
The event started with self introduction of the emcees Lyssy Alex and Dr. Solymole Kuruvilla. Reena Sabu sang a prayer song followed by American national anthem by Ashley Anthony and Indian national anthem by Reena Sabu and Rosy Mathew. The people were entertained with action song by George, Theresa, Catherine, Jacob, Hanna, Krystal, Santana and Aarin. Sherly Sebastian and Bency Jamie sang solo songs. Group dances were performed by Ashley Pulinthanathu, Ashlin Benny, Tessa Lalson, Isabel Jacob, Nicole Manalil, Veena, Ashley and Tina. Ashwin Antony performed an instrumental music. Lyssy Alex and Dr. Solymole Kuruvilla, the emcees, moderated the programs smoothly and efficiently. People used the lunchtime for extended networking.
Recent research makes it clear that any amount of drinking can be detrimental. Here’s why you may want to cut down on your consumption beyond Dry January.
Sorry to be a buzz-kill, but that nightly glass or two of wine is not improving your health.
After decades of confusing and sometimes contradictory research (too much alcohol is bad for you but a little bit is good; some types of alcohol are better for you than others; just kidding, it’s all bad), the picture is becoming clearer: Even small amounts of alcohol can have health consequences.
Research published in November revealed that between 2015 and 2019, excessive alcohol use resulted in roughly 140,000 deaths per year in the United States. About 40 percent of those deaths had acute causes, like car crashes, poisonings and homicides. But the majority were caused by chronic conditions attributed to alcohol, such as liver disease, cancer and heart disease.
When experts talk about the dire health consequences linked to excessive alcohol use, people often assume that it’s directed at individuals who have an alcohol use disorder. But the health risks from drinking can come from moderate consumption as well.
“Risk starts to go up well below levels where people would think, ‘Oh, that person has an alcohol problem,’” said Dr. Tim Naimi, director of the University of Victoria’s Canadian Institute for Substance Use Research. “Alcohol is harmful to the health starting at very low levels.”
If you’re wondering whether you should cut back on your drinking, here’s what to know about when and how alcohol impacts your health.
How do I know if I’m drinking too much?
“Excessive alcohol use” technically means anything above the U.S. Dietary Guidelines’ recommended daily limits. That’s more than two drinks a day for men and more than one drink a day for women.
There is also emerging evidence “that there are risks even within these levels, especially for certain types of cancer and some forms of cardiovascular disease,” said Marissa Esser, who leads the alcohol program at the Centers for Disease Control and Prevention.
The recommended daily limits are not meant to be averaged over a week, either. In other words, if you abstain Monday through Thursday and have two or three drinks a night on the weekend, those weekend drinks count as excessive consumption. It’s both the cumulative drinks over time and the amount of alcohol in your system on any one occasion that can cause damage.
Why is alcohol so harmful?
Scientists think that the main way alcohol causes health problems is by damaging DNA. When you drink alcohol, your body metabolizes it into acetaldehyde, a chemical that is toxic to cells. Acetaldehyde both “damages your DNA and prevents your body from repairing the damage,” Dr. Esser explained. “Once your DNA is damaged, then a cell can grow out of control and create a cancer tumor.”
Alcohol also creates oxidative stress, another form of DNA damage that can be particularly harmful to the cells that line blood vessels. Oxidative stress can lead to stiffened arteries, resulting in higher blood pressure and coronary artery disease.
“It fundamentally affects DNA, and that’s why it affects so many organ systems,” Dr. Naimi said. Over the course of a lifetime, chronic consumption “damages tissues over time.”
Isn’t alcohol supposed to be good for your heart?
Alcohol’s effect on the heart is confusing because some studies have claimed that small amounts of alcohol, particularly red wine, can be beneficial. Past research suggested that alcohol raises HDL, the “good” cholesterol, and that resveratrol, an antioxidant found in grapes (and red wine), has heart-protective properties.
However, said Mariann Piano, a professor of nursing at Vanderbilt University, “There’s been a lot of recent evidence that has really challenged the notion of any kind of what we call a cardio-protective or healthy effect of alcohol.”
The idea that a low dose of alcohol was heart healthy likely arose from the fact that people who drink small amounts tend to have other healthy habits, such as exercising, eating plenty of fruits and vegetables and not smoking. In observational studies, the heart benefits of those behaviors might have been erroneously attributed to alcohol, Dr. Piano said.
More recent research has found that even low levels of drinking slightly increase the risk of high blood pressure and heart disease, and the risk goes up dramatically for people who drink excessively. The good news is that when people stop drinking or just cut back, their blood pressure goes down. Alcohol is also linked to an abnormal heart rhythm, known as atrial fibrillation, which raises the risk of blood clots and stroke.
Newswise — When people are in a negative mood, they may be quicker to spot inconsistencies in things they read, a new University of Arizona-led study suggests.
The study, published in Frontiers in Communication, builds on existing research on how the brain processes language.
Vicky Lai, a UArizona assistant professor of psychology and cognitive science, worked with collaborators in the Netherlands to explore how people’s brains react to language when they are in a happy mood versus a negative mood.
“Mood and language seem to be supported by different brain networks. But we have one brain, and the two are processed in the same brain, so there is a lot of interaction going on,” Lai said. “We show that when people are in a negative mood, they are more careful and analytical. They scrutinize what’s actually stated in a text, and they don’t just fall back on their default world knowledge.”
Lai and her study co-authors set out to manipulate study participants’ moods by showing them clips from a sad movie – “Sophie’s Choice” – or a funny television show – “Friends.” A computerized survey was used to evaluate participants’ moods before and after watching the clips. While the funny clips did not impact participants’ moods, the sad clips succeeded in putting participants in a more negative mood, the researchers found.
The participants then listened to a series of emotionally neutral audio recordings of four-sentence stories that each contained a “critical sentence” that either supported or violated default, or familiar, word knowledge. That sentence was displayed one word at a time on a computer screen, while participants’ brain waves were monitored by EEG, a test that measures brain waves.
For example, the researchers presented study participants with a story about driving at night that ended with the critical sentence “With the lights on, you can see more.” In a separate story about stargazing, the same critical sentence was altered to read “With the lights on, you can see less.” Although that statement is accurate in the context of stargazing, the idea that turning on the lights would cause a person to see less is a much less familiar concept that defies default knowledge.
The researchers also presented versions of the stories in which the critical sentences were swapped so that they did not fit the context of the story. For example, the story about driving at night would include the sentence “With the lights on, you can see less.”
They then looked at how the brain reacted to the inconsistencies, depending on mood.
They found that when participants were in a negative mood, based on their survey responses, they showed a type of brain activity closely associated with re-analysis.
“We show that mood matters, and perhaps when we do some tasks we should pay attention to our mood,” Lai said. “If we’re in a bad mood, maybe we should do things that are more detail-oriented, such as proofreading.”
Study participants completed the experiment twice – once in the negative mood condition and once in the happy mood condition. Each trial took place one week apart, with the same stories presented each time.
“These are the same stories, but in different moods, the brain sees them differently, with the sad mood being the more analytical mood,” Lai said.
The study was conducted in the Netherlands; participants were native Dutch speakers, and the study was conducted in Dutch. But Lai believes their findings translate across languages and cultures.
By design, the study participants were all women, because Lai and her colleagues wanted to align their study with existing literature that was limited to female participants. Lai said future studies should include more diverse gender representation.
In the meantime, Lai and her colleagues say mood may affect us in more ways than we previously realized.
Researcher Jos van Berkum of the Netherlands’ Utrecht University, co-authored the study with Lai and Peter Hagoort of the Max Planck Institute for Psycholinguistics in the Netherlands.
“When thinking about how mood affects them, many people just consider things like being grumpy, eating more ice cream, or – at best – interpreting somebody else’s talk in a biased way,” van Berkum said. “But there’s much more going on, also in unexpected corners of our minds. That’s really interesting. Imagine your laptop being more or less precise as a function of its battery level – that’s unthinkable. But in human information processing, and presumably also in (information processing) of related species, something like that seems to be going on.”
(New Delhi, India: January 11, 2023) “After the highly successful Global Healthcare Summit in Visakhapatnam last weekend, I am happy to announce that the 17th annual Global Healthcare Summit will be held in New Delhi from January 2nd to 4th, 2024,” Dr. Anjana Samadder, President-Elect of the American Association of Physicians of Indian Origin (AAPI) announced here during a Curtain Raiser held at the prestigious Constitution Club in New Delhi on January 9th, 2023.
Organized under the leadership of Dr. Udaya Shivangi, Women’s Forum Chair of AAPI, the kickoff event and press conference was attended by nearly 50 journalists from the nation’s capital and several leaders of APPI, who had come all the way from the United States to be part of this important ceremony. Prominent among those who attended the event included Dr. Seema Arora, past BOT Chair of AAPI, Dr. Raghu Lolabhattu, vice chair of AAPI BOT, Dr. Sreeni Gangasani, Dr. Gautam Samadder, past president of AAPI, Dr. Amit Chakrabarty, Dr. Raj Bhayani, and Dr. Joseph Chalil. Dr. Sampat Shivangi, Chair of AAPI’s Legislative Chair joined the meeting through a message of felicitation sent to the media and AAPI leadership.
In her address, Dr. Anjana Samadder said, the theme for the next global healthcare summit will be “Maa Bachao,” meaning, protecting the mother, which will be a great way to strengthen families and humanity as a whole.
Dr. Sushi Singh, chief guest at the event said, saving the mother and giving her due respect and honor is essential today more than ever. She pointed to the high infant mortality rate in India and urged all sections of society to work together to save girl children.
Picture : TheUNN
Shri. Karthikeyan, a decorated former IPS Officer, in his keynote address, shared of the many sacrifices and contributions by the fraternity of doctors, and lauded them for their services to humanity, especially during the covid pandemic. He shared with the audience his personal experiences working with the most vulnerable people across society and urged everyone to work compassionately towards the poor and help uplift their lives.
In a message, Dr. Ravi Kolli, president of AAPI said, “The Global Healthcare Summit held annually in India across several states, has become a major contributing factor, where Indian American Doctors focus on various programs and policies in their efforts to make a huge difference in the delivery of healthcare in India.”
“Coming from a nation that has given us so much, today Physicians of Indian origin have become a powerful influence in healthcare across the world,” said Dr. Shivangi. “Nowhere in the world is their authority more keenly felt than in the United States. The overrepresentation of Indians in the field of medicine is striking – in practical terms, one out of seven doctors in the United States is of Indian Heritage. We provide medical care to over 40 million of the US population.”
During an interactive session with the media persons who had filled the meeting venue, the leaders of AAPI shared with them of the numerous initiatives taken up by AAPI during the course of the past four decades in India as well as in the United States.
“We the physicians of Indian origin are proud of our great achievements and contributions to our motherland, India, our adopted land, the US, and in a very significant way to the transformation of Indo-US relations and help India to have a cost-effective, efficient and advanced healthcare delivery benefitting India’s 1.4 billion people,” they pointed out.
The Global Health Summit held annually in India has been a major contributing factor by Indian American Doctors, focusing on various programs and policies, and making a difference in the delivery of healthcare in India.
In addition to educational seminars/workshops on current topics, the GHS includes a well-organized CEO forum with a panel of eminent healthcare leaders from the US and India, reinforcing the need for preventive care rather than disease management, to control the non-communicable diseases which are the biggest silent killers.
Areas of ongoing skill training, investment in infrastructure, modernizing healthcare delivery, and private-public collaboration specific to each state in the healthcare sector are discussed and specific plans laid out, which are sent in a White Paper report for follow up in the coming months.
Over the past 17 years and beyond, AAPI leadership has been able to establish Collaboration and multiple medical organizations – ACP – FSMB – ECFMG – NMC (India) – IMA (India) – GAPIO – UNICEF – Red Cross Society – CWC – Lifestyle Medicine – MDTok – Apollo Groups, only to name a few. These connections and collaborations are vital for us to stay connected and make a powerful impact on our communities.
Picture : TheUNN
Through AAPI’s charitable activities with service to our motherland as the motto, AAPI has several programs in India and the United States. Despite the Covid challenges of Delta and Omicron waves, in spite of limited resources, AAPI blood donation drives were done in several cities with several of them organizing multiple events. .
Among several other initiatives, AAPI’s “Adopt a village” Rural Preventive Healthcare Screening Initiative in India, where free health screening camps with free physician consultations were done in several Indian rural villages in the middle of Covid pandemic.
Continuing the efforts towards the Covid-19 Fund – Post-Covid Relief Activities, AAPI has raised over $5 million during the delta wave in India. The ongoing Covid-19 relief work in India is in progress, donating lifesaving equipment to support critically ill patients – Biochemical Analyzers, Ventilators, Oxygen Flow Meters, and Oxygen Plants. The funds will continue to support Covid patients in rural hospitals.
Since its inception 40 years ago, AAPI has served as a link to foster stronger US-India relations and has been lauded by the governments of both nations for their great achievements and contributions.
While proposing vote of thanks, Dr. Gautam Samadder, former President of AAPI said, “Thank you very much for attending the press conference . We appreciate all the efforts media does to promote awareness including health care.
we do hope you will be a integral part of the actual conference next year.”
“We urge you to be part of this event in January 2024 and help create awareness and reach our services to the neediest in India and the United States,” said Dr. Anjana Samadder. For more details about AAPI and its many noble initiatives, please visit: www.aapiusa.org
Dr. Soumya Swaminathan, former World Health Organization (WHO) chief scientist was conferred with the prestigious Prof P. Brahmayya Sastry Oration & Dr. T. Ravi Raju Excellence Award during the 16th Annual Global Healthcare Summit organized by the American Association of Physicians of Indian Origin (AAPI) in Visakhapatnam on Friday, January 6, 2023.
The event jointly organized by Prof P. Brahmayya Sastry Memorial Oration Committee and Andhra Medical College, Visakhapatnam was chaired by Dr. Abhijat Sheth and Dr. Sridhar Chilimuri. While introducing the awardee, Dr. T. Ravi Raju, Chair of the Oration Committee said, Dr. Soumya Swaminathan was most recently WHO’s Deputy Director-General for Programs. A pediatrician from India and a globally recognized researcher on tuberculosis and HIV, she brings with her 30 years of experience in clinical care and research and has worked throughout her career to translate research into impactful programs.
Picture : TheUNN
Dr. Swaminathan was Secretary to the Government of India for Health Research and Director General of the Indian Council of Medical Research from 2015 to 2017. In that position, she focused on bringing science and evidence into health policy making, building research capacity in Indian medical schools and forging south-south partnerships in health sciences. From 2009 to 2011, she also served as Coordinator of the UNICEF/UNDP/World Bank/WHO Special Program for Research and Training in Tropical Diseases in Geneva.
In her eloquent address, Dr. Swaminathan said, “The coronavirus has evolved significantly since it was first traced in late 2019. From being a considerably deadly virus, it has now become less fatal – thanks to the vaccination initiatives across the world.” She asserted that death rates are much higher in unvaccinated compared to vaccinated and boosted individuals.
Dr. Swaminathan, while describing the main lesson from the pandemic, stated that “climate change, and it all boils down to what humans have done to the environment. Our lives are intertwined with the health of the environment,” she added.
Picture : TheUNN
The vulnerable suffer a lot, and it’s important to focus on equity and help those who are left behind, she said. She also stressed on the importance of a public health approach, having good data, and research.
We are recovering quickly because of vaccines, she said, pointing out that over 13 billion people worldwide have taken the vaccine and 20 million lives have been saved due to it. The majority of deaths in the US were because of no vaccination, she added.
Dr Swaminathan further explained that vaccines are developed with high efficacy and safety. The virus is trying to evolve, and each time mutations have allowed the virus to evade antibodies, she said, adding that, “there are people who have not taken the vaccine and haven’t fallen sick, but that’s a matter of chance.
COVID-19 has also disrupted the education system. It has also adversely affected access to nutritious food as a huge number of children depend on school meals, she said and urged everyone to help children overcome and regain the loss they had to endure due to the covid.
Stating that the global pandemic is marching on, the world renowned scientist said, “Of the lessons I have learned since the pandemic began, the most important one is the significance of investing in public health and primary healthcare. Countries that invested in primary healthcare over the past decade or two are reaping the benefits now. Another lesson is the positive role of science and scientists. The global collaboration between scientists to take forward advances in knowledge so that science is continuously informing our response to the pandemic has been encouraging.”
Emphasizing the need for partnership between the private and public sectors, Dr. Swaminathan said, “We also need to think about working with the private sector, which is already playing a very big role in technology. But we need to think about technologies that are considered public health goods.”
For the future, Dr. Swaminathan stressed, “We need to invest in strong institutional mechanisms and capacities in our regulatory bodies, research centers and public health institutions. We have seen so much fear, stigma and discrimination circulated on social media. This must be countered by health literacy.”
Dr. Ravi Kolli, president of AAPI praised the accomplishments and contributions of Dr. Swaminathan and numerous healthcare leaders of Indian origin who have contributed immensely to the many ways, the world has been able to overcome the once in a century, deadly pandemic that has devastated the entire humanity. Expressing hope for the future, he said, “The world looks towards us with hope for leadership and consolidated action to prevent and secure health and well being of everyone committed to our care.”
(Visakhapatnam, India: January 6th, 2023) The 16th annual Global Healthcare Summit (GHS) organized by the American Association of Physicians of Indian Origin (AAPI) was inaugurated with a beautiful rendition of Vande Mataram and the lighting of the traditional lamp by the Chief Guest, Smt. Vidadala Rajini, Honorable Minister for Health, Family Welfare & Medical Education and several other dignitaries, AAPI leaders and local organizers of the Summit at Hotel Novotel on the seashore in Visakhapatnam on January 6th, 2023.
Picture : TheUNN
Attended by nearly 500 delegates from the United States and India, the GHS 2023 is being jointly organized by AAPI and the local organizing committee at Visakhapatnam from January 6th to 8th, 2023. This Global Health Care Summit, with participation from leading medical professionals, thought leaders, heads of several health industry sectors, and policy-makers assumes importance especially in the context of the waning pandemic that has shaken the entire human race and has been instrumental in helping everyone realize that the predicament is common across all the continents.
Shri. YS Jagan Mohan Reddy, Honorable Chief Minister of Andhra Pradesh, in a message delivered to the AAPI delegates at the GHS, urged the members of “the American Association of Physicians of Indian origin to give back something to the society, which has given them an opportunity to pursue medical education and become successful in India and abroad.”
Shri. Jagan Mohan Reddy expressed confidence, stating, “I’m sure this platform will bring together best in the healthcare field from professionals, who will provide innovative solutions for the challenges being faced by all.” Lauding the world-renowned specialists from the United States, who have assembled in Visakhapatnam, Shri Jagan Reddy said, “I am informed that many specialists from the US are attending the conference, whose expertise will be very much useful since their ideas on technology and advances in various fields in solving health related issues in India. While this conference is focusing on mental health, neurology, maternal and child health, oncology, gastroenterology, neurology, cardiology, they will be very relevant to learn from the successful practices abroad.”
Picture : TheUNN
Chief Guest at the Summit, Smt. Vidadala Rajini, Honorable Minister for Health, Family Welfare & Medical Education, said, “The Global Healthcare Summit is an important opportunity for all the healthcare professionals to learn from each other and enhance fellowship. I’m grateful to have this opportunity to attend and learn from all of you,” she said. “I believe that by working with you, we can improve the health and wellbeing of the people in the state. The government has the ability to design the best policies on healthcare, while delivering the best of the patient’s treatment eventually falls into the hands of the physicians.” She praised AAPI delegates for their “dedication and passion to deliver the best patient care. Thank you all once again. The nation is indebted to you for your leadership, and for helping our vulnerable people.” The state has already started taking measures to improve the performance of the healthcare sector by mapping the public healthcare and preventive healthcare system through effective interventions, she said.
While presenting a robust picture of how the state of Andhra Pradesh has become a role model in healthcare delivery with higher rate of investment on healthcare, the Health Minister of Andhra Pradesh said, “Thank you all for being here. And thank you for taking time and conducting such big summits over here. And likewise, it’s a learning session for all of us. And all of your ideas will be taken into consideration by the government of Andhra Pradesh, and let’s all work together and be a part of the growth story of us today.”
Others who spoke on the occasion and felicitated AAPI and the local organizers of the Summit included, Shri. Gudivada Amarnath, Honorable Minister for IT.
Dr Ravi Kolli, President of AAPI in his opening remarks, while describing the objectives of the Summit, said, “The Global Healthcare Summit aims at raising awareness on key health care issues affecting the Indian subcontinent such as Diabetes, Cardiovascular Diseases, Women’s and Children’s Health, Infectious Diseases and Mental Health.” Highlight of this Summit is to reaffirm NRI Physicians’ commitment towards improving health care and create model programs for management of various diseases and to improve outcomes universally, he added. The Summit will be focusing on mental health, reduce the stigma for seeking mental health services, working on Physicians burnout, he added. In addition, AAPI is keen to collaborate with various state and federal government programs to enhance the quality of healthcare delivery, making it affordable, efficient, and equitable, especially helping with the management of various diseases, improving health outcomes universally, training the trainer sessions involving learning modules in different specialties, and tele-consultations.
“We are sure that the Summit will offer a rewarding experience not only on intellectual but on aesthetic front as well, as the scenic beauty of Visakhapatnam and the many places around will be worth going during your trip. The organizing committee is immensely pleased to be at your service,” said Dr. Ravi Raju, Chair of GHS (India) 2023.
Describing some of the objectives of the GHS, Dr. Prasad Chalasani, Chair of GHS (USA) 2023 said. “We hope to create an intellectually charged platform for experts to share their experiences on some of the common professional issues that still remain a challenge in spite of all the advancement. The exchange of expertise and transfer of technology by the best brains is bound to offer positive and innovative solutions to some of the problems faced by humankind.”
Among the many initiatives that emerge from GHS 2023, a notable action plan will be for AAPI to collaborate with the Government of Andhra Pradesh to initiate an ambitious program to address mental health and wellness of students in high school in Andhra Pradesh. Some of the other initiatives that will be announced during the GHS 2023 include: effective treatment modalities on non-communicable medical diseases, reducing the infant and maternal mortality and HPV Vaccination.
Discussions and deliberations that are being addressed included, the Stigma of Mental illness, Suicide prevention, Management of Chronic diseases and Non Communicable Diseases, and other Global Health issues including Climate Change and its impact on health.
The essence of AAPI is educational. That translates into numerous Continuing Medical Education and non-CME seminars by experts in their fields. The GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” has several CME sessions that focus on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, and Medical Jeopardy.
CME sessions with academicians from the United States offer unique opportunities for local medical staff and healthcare professionals to advance leanings and provide the best possible care for the people of India. The Summit will have a research competition for medical students and post graduate students from all over India. AAPI will confer Awards of excellence and lifetime achievements during the Summit.
“In our quest to fulfill the mission of AAPI, we are proud to share best practices and experiences from leading experts in the world and develop actionable plans and projects that enable access to affordable and quality healthcare for all people. To help accomplish this mission, we are excited to be here in Visakhapatnam and be part of the GHS 2023,” Dr. Kolli urged. For more information on Global Health Summit, please visit: www.summit.aapiusa.org and www.GHS2023.com
we are excited to be here in Visakhapatnam and be part of the GHS 2023,” Dr. Kolli urged. For more information on Global Health Summit, please visit: www.summit.aapiusa.org and www.GHS2023.com
The director of the George Washington University School of Medicine argues that the brain of an older person is much more practical than is commonly believed. At this age, the interaction of the right and left hemispheres of the brain becomes harmonious, which expands our creative possibilities. That is why among people over 60 years of age you can find many personalities who have just started their creative activities.
Of course, the brain is no longer as fast as it was in youth. However, it gains in flexibility. Therefore, with age, we are more likely to make the right decisions and are less exposed to negative emotions. The peak of human intellectual activity occurs around the age of 70, when the brain begins to function at full strength.
Over time, the amount of myelin in the brain increases, a substance that facilitates the rapid passage of signals between neurons. Due to this, intellectual abilities increase by 300% compared to the average.
Also interesting is the fact that after 60 years, a person can use 2 hemispheres at the same time. This allows you to solve much more complex problems.
Picture : NIH
Professor Monchi Uri, from the University of Montreal, believes that the old man’s brain chooses the path that consumes less energy, eliminates the unnecessary and leaves only the right options to solve the problem. A study was conducted involving different age groups. Young people were very confused when passing the tests, while those over 60 years of age made the right decisions.
Now, let’s look at the characteristics of the brain between the ages of 60 and 80. They are really pink. *CHARACTERISTICS OF THE BRAIN OF AN ELDERLY PERSON.*
Neurons in the brain do not die, as everyone around you says. The connections between them simply disappear if one does not engage in mental work.
Distraction and forgetfulness arise due to an overabundance of information. Therefore, it is not necessary for you to concentrate your whole life on unnecessary trifles.
From the age of 60, a person, when making decisions, does not use one hemisphere at the same time, like young people, but both.
Conclusion: if a person leads a healthy lifestyle, moves, has viable physical activity and is fully mentally active, intellectual abilities do NOT decrease with age, they simply GROW, reaching a peak at the age of 80-90 years .
So do not be afraid of old age. Strive to develop intellectually. Learn new crafts, make music, learn to play musical instruments, paint pictures! Dance! Take an interest in life, meet and communicate with friends, plan for the future, travel as best you can. Do not forget to go to shops, cafes, shows. Don’t shut up alone, it’s destructive to anyone. Live with the thought: all good things are still ahead of me! (SOURCE: New England Journal of Medicine)
The growing influence of physicians of Indian heritage is evident, as they are increasingly recognized and hold critical positions in healthcare, academic, research, and administrative positions across the nation. With their hard work, dedication, compassion, and skills, they have thus carved an enviable niche in the American medical community. Not satisfied with their own professional growth and the service they provide to their patients around the world, they are in the forefront, sharing their knowledge and expertise with others, especially those physicians and leaders in the medical field from India.
Picture : TheUNN
The 16th annual Global Healthcare Summit (GHS) 2023, organized by the Association of American Physicians of Indian Origin (AAPI) in Visakhapatnam in the state of Andhra Pradesh from January 6th to 8th, 2023 offers a unique forum for them to come together, sharing their knowledge and expertise with their fellow physicians from around the world, and to learn from one another.
According to Dr. Ravi Kolli, President of AAPI, “AAPI has been engaged in harnessing the power of Indian Diaspora to bring the most innovative, efficient, cost-effective healthcare solutions to India. The upcoming GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” with its focus on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, Medical Jeopardy, and Research Poster presentations by medical students will be a great way to accomplish this mission of AAPI. In addition, advocacy to dismantle the stigma of mental illness and Suicide Prevention will be the highlight of the program.”
“This conference will focus on bringing the highest caliber of internationally acclaimed faculty and will develop a very robust agenda in collaboration with leading experts from India. The enhanced focus on conducting skills enhancement workshops, hands on experience with advanced techniques,” Dr. V. Ranga, Chair of AAPI BOT said.
CME sessions with academicians from the United States will offer unique opportunities for local medical staff and healthcare professionals to advance leanings and provide the best possible care for the people of India. Nearly 400 Physicians are expected to attend the AAPI GHS 2023.
Picture : TheUNN
Invited guests include Professors, Heads of Educational Institutes, Deans as well as chairs and members of the National Medical Council Board, in addition to the dignitaries, including Hon. Health Minister of India, Hon. Chief Minister and the Hon. Governor of Andhra Pradesh and Telangana. Sponsors will have opportunities for Exhibits, Product Theaters, NGO booths to promote their services, products, and values.
Dr. Prasad Chalasani, Chair of AAPI GHS-USA says, “The scientific program and workshops of GHS is developed by leading experts with contributions from the Scientific Advisory Board and the International Scientific Committee. The workshops will be led by world-famous physicians on topics relevant to the needs of the time.”
“AAPI has plans to collaborate with the Government of Andhra Pradesh to initiate a very ambitious program to address mental health and wellness of all the students in the high schools in AP,” Dr. Ravi Raju, Chair of GHS-India said.
Discussions and deliberations will address the Stigma of Mental illness, Suicide prevention, Management of Chronic diseases and NCD and, other Global Health Issues including Climate Change and its impact on health will be discussed.
Dr. Sampath Shivangi, AAPI Legislative Committee Chair said, “We are collaborating with senior leaders from leading healthcare organizations including pharmaceuticals, device and medical equipment manufacturers and major medical teaching institutions, hospitals, and the Ministries of Health, External/Overseas Affairs and regulatory bodies to attend and coordinate with AAPI with an ultimate goal to providing accessible and affordable high-quality healthcare to all people of India.”
Dr. Manoj Jain,Chair of CETI – Collaboration to Eliminate TB in India supported by CDC and USAIDwill lead comprehensive discussions on the TB Elimination Projects in India, with tangible goals achieved and the plan for the future.
Dr. Sreeni Gangasani, CME Chair, and Academic Chair Dr. Sharma Prabhakar said, some of the topics for the CMEs will include Psychiatry, Ophthalmology, Pediatrics, Gastroenterology, Neurology, and Oncology. “In our efforts to realize the core mission of AAPI, which is to share the best from leading experts from around the world, to collaborate on clinical challenges, the GHS in Visakhapatnam will have clinical tracks that are of vital to healthcare in India,” Dr. Gangasani added.
Dr. Lokesh Edara and Dr. Brahma Sharma, who are the co-chairs of International medical education will conduct a high-powered panel discussion by International Medical Education experts including CEOs of ECFMG, WFMC, and National Medical Council officials. Dr. B K Kishore, an academic expert will lead discussions on research methodology and scientific writings. Latest Advances, CME, ENLS, Discussions on Research Methodology and Scientific Writing by Academic Experts will be part of the summit.
According to Dr. Joseph Chalil, Chair of AAPI’s CEO Forum and Strategic Advisor, “The CEO forum will focus on Equity, Ethics and Physician Burnout Issues” while the Women’s Forum chair, Dr. Udaya Shivangi said, “Women’s Forum will focus on empowerment, gender bias and leadership.”
Walkathon on the beach will be held to challenge mental health stigma and promotion of healthy lifestyle changes and stress management of and several other initiatives also will be announced including effective treatment modalities on non-communicable medical diseases, reducing the infant and maternal mortality and HPV Vaccination.
The Summit will have a research competition for medical students and post graduate students from all over India. AAPI will confer Awards of excellence and lifetime achievements. “AAPI will work collaboratively with GAIMS – Global Association of Indian Medical Students and will be conducting the Research Competition for Medical, Students, Residents, Fellows, and Junior Doctors,” said Dr. Anjana Samadder, President-Elect of AAPI.
“With the changing trends and statistics in healthcare, both in India and US, we are refocusing our mission and vision, AAPI will continue to make a positive meaningful impact on the healthcare delivery system both in the US and in India,” said Dr. Satheesh Kathula, Vice President of AAPI.
“January is #CervicalCancer Awareness Month! In coordination with the local organizers of the GHS, AAPI will continue its efforts to create awareness and offer financial assistance to eradicate this preventable disease,” said Dr. Meher Medavaram, Secretary of AAPI. “AAPI’s this new initiative through education and awareness programs is aimed at helping save millions of lives in India,” she added.
Dr. Sumul Rawal, Treasurer of AAPI pointed out, “India needs to redouble and continue its efforts and dedicate resources to tackle the perennial health challenges. Many of these projects and programs need regular funding and management of resources. We are grateful to dozens of AAPI members who have committed to serving India with an ongoing commitment.”
This international healthcare summit is a progressive transformation from the first Indo-US Healthcare Summit launched by AAPI USA in 2007. With the objective of enabling people in India to access high-quality, affordable, and cost-effective world-class health services, the Summit to be held in collaboration with the Indian Medical Association (IMA), the Ministry of Overseas Indian Affairs & the Ministry of Health, will have participation from some of the world’s most well-known physicians and industry leaders.
The scientific program of GHS 2023 is developed by leading experts with the contributions of a stellar Scientific Advisory Board, Continuing Medical Education Committee and Academic Committee of AAPI and Indian counterparts. The Conference in collaboration with several professional associations from all over the world, 12 hours of credits from the Accreditation Council for Continuing Medical Education.
“With the changing trends and statistics in healthcare, both in India and US, we are refocusing our mission and vision of GHS 2023, and AAPI would like to make a positive and meaningful impact on the healthcare in India,” Dr. Kolli says. “In our quest to fulfill the mission of AAPI, we are proud to share best practices and experiences from leading experts in the world and develop actionable plans and projects that enable access to affordable and quality healthcare for all people. To help accomplish this mission, please join us at the GHS 2023.” For more information on Global Health Summit, please visit: www.summit.aapiusa.org and www.GHS2023.com
(AP) — Long before the bobbleheads and the “Fauci ouchie,” Dr. Anthony Fauci was a straight-shooter about scary diseases — and “stick with the science” remains his mantra.
Fauci steps down from a five-decade career in public service at the end of the month, one shaped by the HIV pandemic early on and the COVID-19 pandemic at the end.
In an interview with The Associated Press, Fauci said he leaves excited by the prospect of advances such as next-generation coronavirus vaccines — but worried that misinformation and outright lies mark a “profoundly dangerous” time for public health and science.
“Untruths abound and we almost normalize untruths,” Fauci said. “I worry about my own field of health, but I also worry about the country.”
Fauci, who turns 82 on Christmas Eve, has been a physician-scientist at the National Institute of Allergy and Infectious Diseases for 54 years, and its director for 38 of them.
Picture : AP
Because he candidly puts complex science into plain English, Fauci has advised seven presidents, from Ronald Reagan to Joe Biden, about a long list of outbreaks — HIV, Ebola, Zika, bird flu, pandemic flu, even the 2001 anthrax attacks.
“Stick with the science and never be afraid to tell somebody something that is the truth — but it’s an inconvenient truth in which there might be the possibility of the messenger getting shot,” Fauci said. “You don’t worry about that. You just keep telling the truth.”
He added, with characteristic understatement: “That’s served me really quite well with one exception that, you know, the truth generated a lot of hostility towards me in one administration.”
For all his prior influence on national and even global responses to infectious diseases, it wasn’t until COVID-19 paralyzed the world in early 2020 that Fauci became a household name — giving the latest updates at daily White House press conferences and in frequent media interviews.
But eventually, Fauci found himself having to contradict then-President Donald Trump’s attempts to downplay the severity of the viral threat and promote unproven treatments. Trump and his allies began attacking Fauci, who even received death threats that required a security detail for his protection.
As the world enters another year of COVID-19, Fauci still is a frequent target of the far right — but also remains a trusted voice for millions of Americans.
Under his watch, researchers at the National Institutes of Health laid the scientific groundwork for the speedy development of powerful coronavirus vaccines. An analysis released by the Commonwealth Fund last week found the shots saved 3.2 million lives in the U.S. alone and prevented 18.5 million hospitalizations.
With another winter uptick underway, Fauci’s disappointed that just 14% of people eligible for the updated COVID-19 boosters — shots that add protection against omicron strains — have gotten one.
“That doesn’t make any sense at all, when you have a vaccine that you know is life-saving,” he said. But he’s also looking forward to next-generation vaccines that do a better job of preventing infection, citing promising leads like nasal vaccines.
For all the political attacks, the public did struggle to understand why some of his and others’ health advice changed as the pandemic wore on — such as why masks first were deemed unnecessary and later mandated in certain places.
Fauci said one of the pandemic’s lessons is to better convey that it’s normal for messages to change as scientists make new discoveries. “That doesn’t mean you’re flip-flopping. That means you’re actually following the science,” he said.
Fauci has had a hand in life-saving scientific advances for decades. As a young researcher at the National Institutes of Health, he helped develop highly effective therapies for rare but once-fatal blood vessel diseases known as vasculitis syndromes.
Then came the AIDS crisis and days that Fauci, treating patients in NIH’s hospital, recalled as “very dark and very difficult. As a physician you’re trained to heal people. And we weren’t healing anybody. Everybody was dying in front of us.”
Fauci created an AIDS division that, together with drug companies and universities, led research into drugs that eventually transformed HIV into a manageable chronic disease. Later, under President George W. Bush, Fauci helped develop PEPFAR, the President’s Emergency Plan for AIDS Relief, to bring those HIV medications to poor countries. The program is credited with saving more than 20 million lives over the past 20 years.
But it took years to get even the first anti-AIDS medications — and in the late 1980s and early ’90s, furious activists protested what they saw as government indifference. Fauci brought the activists to the table, making it standard practice for patient advocates to have a voice in government decisions about drug research. Unfortunately, he said, that experience can’t help bridge today’s political divisions that are hurting public health.
The AIDS activists “were theatrical. They were iconoclastic. They were provocative. They were confrontational, all of the above. But the fundamental core message that they had was a correct message,” Fauci said. “That is enormously different from what is going on right now with COVID, where untruths abound, conspiracy theories abound, distortions of reality abound.”
A team of Indian scientists has developed a breakthrough output in collaboration with Atlanta’s Emory University—a coronavirus countering unique monoclonal antibody that effectively neutralizes a wide range of COVID-19 variants.
The collaboration between the scientists at the Delhi-based International Centre for Genetic Engineering and Biotechnology (ICGEB), funded by the ICMR and Emory Vaccine Center (EVC) effectively neutralizes a wide range of SARS-CoV-2 variants including Alpha, Beta, Gamma, and the different Omicron sub-lineages including, BA.1, BA.2 and others., Dr. Rafi Ahmed, Director, Emory Vaccine Center, told NRI Pulse. The antibody has been tagged 002-S21F2.
002-S21F2 is a dream come true for scientists and researchers who, since the emergence of the pandemic, have been in pursuit of a single antibody that can fight not only one strain of the virus but subsequent variants.
Dr. Ahmed says, is a result of research carried out on patients in India who had mild cases of the original Wuhan strain of Covid-19. The collaborative research was carried out by ICGEB in partnership with the National Institute of Malaria Research (ICMR-NIMR, New Delhi) working with the Emory Vaccine Center (Atlanta, USA). Dr. Ahmed credits the discovery to Dr. Anmol Chandele, who serves as the Group Lead at ICGEB and resides in Delhi and Dr. Murali-Krishna Kaja, who splits his research time between Atlanta and New Delhi.
The screening of single-cell Memory B cells, the organisms that create lifelong immunity to infecting pathogens, derived from covid-19 recovered patients from India was the base of the research and discovery.
Antibodies target particular cell surfaces and either destroy the infected cell or eradicate the virus from the host. Monoclonal antibody (protein) is produced from a cell line made by cloning a unique white blood cell.
“Scientists at ICGEB generated a batch of over 300 different antibodies that came from different patients in India who were affected by the original Wuhan strain,” Dr Ahmed says. “At the time, there were no new variants. So most of the antibodies that were generated by our lab were able to neutralize the Wuhan strain, and not surprisingly, did not react effectively with other strains, because typically antibodies are very effective against the strain the infected them.”
But the team was lucky. “Two, out of the 300 or so monoclonals we discovered, were broadly cross-reactive, and one antibody, in particular, is a very rare one as described anywhere. It not only neutralized the Wuhan strain but the Delta, Beta and also Omicron and its sub-lineages including, BA.1, BA.2 and many others. And then a group of structural biologists at Emory in Atlanta, with Dr. Anamika Patel and Dr. Eric Ortlund researched reasons to find out why the antibody was so successful in neutralizing all the variants.”
“It turned out that this (antibody) is seeing a very unique part of the spike protein (the spike you see in the pictures everywhere) is what binds to the cellular receptor. So, if that is blocked, the binding is blocked. This monoclonal was seeing it from an angle which was common to all variants and not limited to any one type. It is actually a better monoclonal in terms of any of the other licensed monoclonals across the world. They are not as effective as this one,” Dr. Ahmed elaborated.
Unlike other monoclonal antibodies that target the (virus) areas that are a hotspot for mutation, 002-S21F2 attacks the protein spikes (portion of the virus) that remain the same across all variants. It targets a highly conserved area on the outer surface of the receptor binding domain of the virus, and with 002-S21F2 being broad-spectrum, neutralizes all the known variants. And since it is derived from human strains, tolerance is not an issue.
“We are now hoping is that the Indian government will work with the appropriate pharmaceutical companies in India. This antibody is patented in India, so it can be used in India and produced by a pharmaceutical company in India and we want to ensure that it is not expensive to buy for patients,” Dr. Ahmed notes.
“If produced quickly it could be of great value, particularly in immuno-compromised patients, or someone who is really sick or for people with cancers related to immune systems, lymphoma, multiple myeloma, or transplant patients who are on immunosuppressive regimen who cannot be given vaccines,” he added.
Antibodies cannot be administered to everybody. They have a short half life – meaning they disappear from the body after a few weeks because there is nothing to produce it. While vaccines can be made available to everyone, antibody treatments are the solution to specialized cases with immediate requirements such as immunocompromised cases mentioned above.
AAPI Urges Government to prevent violence and bring to justice those harm Physicians
Chicago, IL: November 29, 2022: “AAPI is very concerned by the recent and ongoing assaults on Doctors and Medical Professionals in India and joins American Kerala Medical Graduates Association (AKMG ) and Kerala Medical Post Graduates Association in condemning the recent physical assault on a female Doctor at Thiruvananthapuram Government Medical College on November 23rd that was caught on the CCTV,” Dr. Ravi Kolli, President of American Association of Physicians of India Origin (AAPI) said here today.
The leadership of AAPI, including Drs. Ravi Kolli, President of AAPI, Dr. Vishweshwar Ranga, Chair, BOT of AAPI, Dr. Raghu Lolabhattu, Vice Chair, AAPI BOT, Dr. Anjana Samadder, President-Elect of AAPI, Dr. Satheesh Kathula, Vice President of AAPI, Dr. Sujeeth Punnam, Chair, Alumni Committee of AAPI, Dr. Geetha Nair, President of AKMG, Dr. Nigil Haroon, immediate past President of AKMG, and Dr. Subra Bhat, past President of AKMG, and the entire Executive Committee and Board Of Trustees of AAPI, stand in solidarity with our fellow physicians and medical professionals, who are on the front line, work very hard, day and night to serve and take care of patients diligently and dutifully, Dr. Kolli said in a statement issued here.
Quoting media reports last month that pointed to a very grim situation in the state of Punjab in India, Dr. Kolli said, it is shocking to learn of “Recent incidents of physical assaults and misconduct have once again instilled a sense of fear in the mind of on-duty medical staff. As per the data, compiled by the Punjab Civil Medical Services (PCMS) Association, over 400 incidents of violence against medical staff, including doctors, have been reported over the past two years.”
Recalling that from ancient times, physicians across the world have been revered for dedicating their lives for the noble mission of preventing people from getting and saving millions of lives of people from illnesses, Dr. Anjana Samadder, President-Elect of AAPI said. “We as a community of physicians and individual members of this fraternity have decided to go into the medical profession with the best of intentions. We as physicians want to help people, ease suffering and save lives. Physicians of Indian origin are well known around the world for their compassion, passion for patient care, medical skills, research, and leadership.”
“We strongly urge both the central and state governments to take decisive and drastic actions to curb these anti-social behaviors that endanger doctors serving patients,” Dr. Ranga, BOT Chair of AAPI said. He agreed with the health experts who “want a multi-pronged approach to prevent such attacks, involving reducing the crowd by strengthening peripheral hospitals, increasing staff and providing better security.”
Dr, Satheesh Kathula, Vice President of AAPI said, “These incidents are unfortunate. We urge the federal and the state governments to provide adequate security at all hospitals and healthcare centers.” AAPI supports the petition calling for justice to the Doctor attacked in Thiruvananthapuram, which has gained support from the Kerala Medical Post Graduate Association, who stated that it is unsettling that such attacks occurred in medical campuses, which are supposed to be a secure location, he added.
“AAPI members share their angst as there is not enough support from the state and federal governments and the larger society as the attacks on Medical Professionals in India continue to rise, Dr. Meher Medavaram, Secretary of AAPI said.
Pointing to the trend of increasing violence against the Medical Professionals, and the actions against the perpetrators are disproportionately low, Dr. Sumul Raval, Treasurer of AAPI said, “Medical Professionals cannot provide the best possible health services to the people until there is a safe working environment. Potential fear of violence always looms, especially in the overcrowded Government Hospitals.”
Several aspiring Physicians have expressed concerns following the assault on the female doctor at Thiruvananthapuram Government Medical College last week. The attacked female Doctor is quoted to have told Dr. Sulphi N, the Indian Medical Association state president, that she was shocked and regretted her decision to pursue a career as a Doctor and even as a neurosurgeon.
“Despite the noble intentions to save lives and prevent pain and suffering among the patients, Doctors and Medical Professionals continue to put their own lives on the line in the course of their jobs, it is shocking that face such attacks from the very people they are trying to help,” Dr. Sujeeth Punnam, Chair, Alumni Committee of AAPI added.
Dr. Raghu Lolabhattu, Vice Chair, AAPI BOT said, “AAPI urges the Government of India and the State Governments across the country to bring to justice those behind the cruel attacks on the physicians who have dedicated lives for serving the sick, especially during the critical Covid pandemic, risking his own life and that of his dear ones.”
“We at AAPI, the largest ethnic medical organization in the United States urge the Government of India and every state in India to make all the efforts needed to prevent violence against medical professionals and enable them to continue to serve the country with dignity, pride and security. We are shocked by the lack of coherent action against such violence and protect members of this noble fraternity. And we want immediate action against the culprits, who have been carrying on these criminal acts.” For more information on AAPI, please visit: www.aapiusa.org
Newswise — When the U.S. Food and Drug Administration gave controversial accelerated approval to the first Alzheimer’s drug in nearly 20 years, it had a surprising impact on attitudes about research into the disease. A survey by University of California, Irvine neuroscientists has found news coverage of the FDA’s decision made the public less willing to volunteer for Alzheimer’s pharmaceutical trials.
Picture : UCI News
The study was conducted by the UCI Institute for Memory Impairments and Neurological Disorders, known as UCI MIND. It appears in the Journal of Alzheimer’s Disease. (Link to abstract: https://content.iospress.com/articles/journal-of-alzheimers-disease/jad220801)
The UCI team performed the survey in tandem with the FDA’s spring 2021 consideration of aducanumab. The monoclonal antibody reduces brain plaques, an Alzheimer’s hallmark, in people with the condition. A panel of outside experts advised the FDA against approval, saying aducanumab’s ability to decrease plaques hadn’t shown an impact on the disease’s clinical progression. The agency’s controversial go-ahead and further disaccord over the drug’s labeling and price captured widespread media attention.
The UCI MIND researchers conducted their study among people aged 50 to 79 who had expressed willingness to take part in drug research. Two weeks before the FDA’s decision, UCI MIND asked respondents if they would be interested in enrolling in a hypothetical four-year study of a plaque-reducing monoclonal antibody and a plaque-preventing drug known as a BACE inhibitor. Eight days after the FDA gave aducanumab the green light, UCI MIND sent survey participants a similar questionnaire with a new section about the monoclonal antibody and its approval.
“We found those who had heard about the FDA decision before our follow up became less willing to take part in a drug trial,” said neurobiology & behavior graduate student Marina Ritchie, corresponding author of the paper. “The people who learned about it from our materials demonstrated absolutely no change in their willingness.”
UCI MIND Director Joshua Grill added: “This is surprising, because it goes against some of our previous data showing people are generally more willing to take part in studies involving approved drugs compared to investigational ones. We believe it could be evidence of the powerful influence of media coverage of science.”
The survey’s findings may offer important insights for Alzheimer’s disease researchers. “Alzheimer’s is the most important medical condition society faces and we need an army of citizen volunteers to participate in drug trials,” said Grill, a professor of neurobiology & behavior and psychiatry & human behavior. “Anything that diminishes credibility in scientific research impedes our progress. Media coverage has the potential to influence people’s choices. That can hold us back or push us forward.”
The findings also show researchers need to be aware of sample bias. It occurs when people with certain characteristics participate in a study at a higher rate than others without those traits or if some research population segments are not fairly represented.
“It’s crucial for trial participants to reflect the scope of people affected by the disease,” Ritchie said. “One thing we don’t know is whether the impact of media attention may be more or less important for particular groups, especially groups underrepresented in research.”
The UCI MIND team plans to conduct further research into the issue, with emphasis on learning how to better ensure diverse populations are part of Alzheimer’s clinical trials. “We need to understand what barriers to trust may exist and overcome them so our research is inclusive and applicable to everyone,” Grill said. Funding for the project was provided by the UCI Alzheimer’s Disease Research Center.
“Lifestyle medicine is the simplest yet most powerful approach to true health and healing,” said Dr. Ravi Kolli, President of the American Association of Physicians of Indian Origin (AAPI) while setting the context for the Lifestyle Medicine & Wellness Webinar organized on November 19th, 2022. “We understand that well-being is more than the absence of disease. It’s our hope that by attending this very important webinar today, we all will experience the transformative power of using everyday choices and habits to achieve peak performance and well-being.”
Dr. Sreeni Gangasani, AAPI’s CME Chair, while welcoming the nearly 200 AAPI members who attended the webinar, introduced Dr. Koushik Reddy, who is passionate and deeply committed to the idea of health promotion and disease prevention, using lifestyle and nutrition-related tools, and, Dr. Param Dedhia, a dedicated internal and integrative medicine practitioner, who is a board-certified Integrative Medicine Physician, Internal Medicine Doctor, Obesity Medicine Expert, and Sleep Medicine Specialist, who led the discussions today on Lifestyle Medicine and Wellness.
“I Have a Carrot and a Stent, You Pick!,” Dr. Koushik R. Reddy, director of interventional cardiology at the James A Haley VA Medical Center in Tampa, FL, challenged a record over 200 Physicians who had joined the webinar on weekend morning. Dr. Kaushik Reddy emphasized the importance of a fundamental diet, physical activity, and other lifestyle approaches in the primordial and primary prevention of many NCDs that can easily be prevented through simple day-to-day choices.
Dr. Koushik Reddy argued that our healthcare system is really a disease management system, but we still have some agency. He shared with AAPI members several pillars he believes will help each of us have a happy, long healthy life. In his address, he said, he is deeply committed to the idea of health promotion and disease prevention, using lifestyle and nutrition-related tools. It is with this passion and commitment, he boldly challenges his patients with – “I have a carrot and a stent, you pick!”
Picture : TheUNN
Dr. Reddy said Lifestyle medicine-certified clinicians are trained to apply evidence-based, whole-person, prescriptive lifestyle change to treat and, when used intensively, often reverse such conditions. Applying the six pillars of lifestyle medicine—a whole-food, plant-predominant eating pattern, physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connections—also provides effective prevention for these conditions. Dr. Reddy discussed the flaws and opportunities inherent in our healthcare system as it relates to heart health. He spoke about the power of plant-based nutrition and lifestyle medicine, and how he incorporates those principles into his current practice.
Both the quality of life and the quantity of life, are inseparable components of a Good Lifestyle, he said. Pointing to how in 1920, the life expectancy was 42, and in 202o, it has nearly doubled to 78. While the quantity of life has increased tremendously, the quality of life has suffered greatly. “While we are living longer, we are also dying longer due to illnesses.” Dr. Reddy pointed out that the United States is not among the healthy nations of the world because “We are failing the system.” In his efforts to spread the message, he said, “I am happy to work with AAPI and help spread the message of Lifestyle Medicine beyond AAPI and to back home in India.”
Dr. Reddy, after practicing interventional cardiology for ten years, changed his focus towards cardiovascular health promotion and disease prevention, using lifestyle and nutrition-based strategies. He is a member of the American College of Cardiology’s working group on nutrition and lifestyle and is board certified in Cardiology, Interventional Cardiology, and Lifestyle Medicine. He is closely involved with the department of Whole Health at the Tampa VA hospital. Working in partnership with the local Whole Health leadership, he established two preventive cardiology clinics. “HEAL – Healthy Eating and Living – Introductory Program. CALM – Comprehensive Approach to Lifestyle Medicine – 6 weeks of the multidisciplinary program.”
In his insightful address on “Sleep, The Master Lever Of Health,” Dr. Param Dedhia, who had his education at Johns Hopkins University and Canyon Ranch, which allowed him to bridge eastern and western philosophies, and connect traditional wisdom to modern science, is the Founder & Medical Director of Moveo Health, a personalized health program focused on longevity, shared at length some valuable lessons and words of wisdom on the importance of staying curious and honoring our health.
Referring to Sleep Medicine in the United States as only 40 years old, Dr. Dedhia stressed the importance of sleep in our daily lives and said, “Sleep is about restoring.” He said, “Sleep evolves through adulthood. So, we must evolve our lifestyles to promote sleep. According to him, “Most adults need 7-9 hours” of sleep daily. In his address, he pointed to the function & promise of sleep, which Restores, and Cools the brain and body. It helps regulate ion channels and optimizes physiological growth. Sleep is Anti-Inflammatory, as it helps reduce inflammatory markers. Sleep improves one’s mood, by soothing emotions & mental fatigue.
Sleep is “Actively cardio-protective and Enhances neuro-plasticity.” Another important function of Sleep is to help “Improve memory formation & consolidation.” Sleep “connects us physically, mentally & emotionally” and helps us “Replete energy stores.”
Dr. Dedhia, who continues to pursue his passion and be an advocate for people to live their best lives, quoting scientific studies and evidence-based research, Dr. Dedhia said, “Rx for optimal sleep & health are: (1) Quantity and (2) Quality, which are determined by ‘Daytime Lifestyle’ and ‘Nighttime Sleep,’ by creating ‘Night Time Rituals’ that last a lifetime.”
Dr. Sreeni Gangasani, AAPI CME Chair, said, with the rapidly worsening trends in Chronic Lifestyle Related Non-communicable diseases across the world stemming from modern food and diet practices, inadequate physical activity, poor sleep, worsening stress, poor social relationships, and risky substances abuse – healthcare systems across the world are now inundated with premature and preventable mortality and morbidity from these NCDs. In this context, “Today’s webinar is filled with inspiring and informative talks and presentations by two great speakers that shed the light on the importance of lifestyle interventions as the primary mode of prevention.
In his vote of thanks, Dr, Pankaj Vu, Director of Lifestyle Medicine at Kaiser Permanente, while expressing gratitude to the internationally renowned speakers for their inspiring discussions on Lifestyle Medicine and for AAPI members for being part of this important session said, said, “In support of physician well-being and self-care, such sessions are being offered to the AAPI members, families and friends.”
In his remarks, Dr. Satheesh Kathula, Vice President of AAPI, while referring to the importance of the Webinar, said, “It is well established that evidence-based clinical nutrition and lifestyle practices play a pivotal role in the prevention, treatment, and potential reversal of various common chronic diseases. However, this area of science is underappreciated at all levels of medical education and training. Most medical schools and residency programs do not offer any organized training in nutrition and lifestyle medicine. Given recent data on the rising cost and loss of quality of life secondary to preventable causes, there is an absolute need for a drastic reform of the US medical education system.” Fort more details on AAPI, please visit: www.aapiusa.org
Chicago, IL: November 29, 2022: “AAPI is very concerned by the recent and ongoing assaults on Doctors and Medical Professionals in India and joins American Kerala Medical Graduates Association (AKMG ) and Kerala Medical Post Graduates Association in condemning the recent physical assault on a female Doctor at Thiruvananthapuram Government Medical College on November 23rd that was caught on the CCTV,” Dr. Ravi Kolli, President of American Association of Physicians of India Origin (AAPI) said here today.
The leadership of AAPI, including Drs. Ravi Kolli, President of AAPI, Dr. Vishweshwar Ranga, Chair, BOT of AAPI, Dr. Raghu Lolabhattu, Vice Chair, AAPI BOT, Dr. Anjana Samadder, President-Elect of AAPI, Dr. Satheesh Kathula, Vice President of AAPI, Dr. Sujeeth Punnam, Chair, Alumni Committee of AAPI, Dr. Geetha Nair, President of AKMG, Dr. Nigil Haroon, immediate past President of AKMG, and Dr. Subra Bhat, past President of AKMG, and the entire Executive Committee and Board Of Trustees of AAPI, stand in solidarity with our fellow physicians and medical professionals, who are on the front line, work very hard, day and night to serve and take care of patients diligently and dutifully, Dr. Kolli said in a statement issued here.
Quoting media reports last month that pointed to a very grim situation in the state of Punjab in India, Dr. Kolli said, it is shocking to learn of “Recent incidents of physical assaults and misconduct have once again instilled a sense of fear in the mind of on-duty medical staff. As per the data, compiled by the Punjab Civil Medical Services (PCMS) Association, over 400 incidents of violence against medical staff, including doctors, have been reported over the past two years.”
Picture : TheUNN
Recalling that from ancient times, physicians across the world have been revered for dedicating their lives for the noble mission of preventing people from getting and saving millions of lives of people from illnesses, Dr. Anjana Samadder, President-Elect of AAPI said. “We as a community of physicians and individual members of this fraternity have decided to go into the medical profession with the best of intentions. We as physicians want to help people, ease suffering and save lives. Physicians of Indian origin are well known around the world for their compassion, passion for patient care, medical skills, research, and leadership.”
“We strongly urge both the central and state governments to take decisive and drastic actions to curb these anti-social behaviors that endanger doctors serving patients,” Dr. Ranga, BOT Chair of AAPI said. He agreed with the health experts who “want a multi-pronged approach to prevent such attacks, involving reducing the crowd by strengthening peripheral hospitals, increasing staff and providing better security.”
Dr, Satheesh Kathula, Vice President of AAPI said, “These incidents are unfortunate. We urge the federal and the state governments to provide adequate security at all hospitals and healthcare centers.” AAPI supports the petition calling for justice to the Doctor attacked in Thiruvananthapuram, which has gained support from the Kerala Medical Post Graduate Association, who stated that it is unsettling that such attacks occurred in medical campuses, which are supposed to be a secure location, he added.
“AAPI members share their angst as there is not enough support from the state and federal governments and the larger society as the attacks on Medical Professionals in India continue to rise, Dr. Meher Medavaram, Secretary of AAPI said.
Pointing to the trend of increasing violence against the Medical Professionals, and the actions against the perpetrators are disproportionately low, Dr. Sumul Raval, Treasurer of AAPI said, “Medical Professionals cannot provide the best possible health services to the people until there is a safe working environment. Potential fear of violence always looms, especially in the overcrowded Government Hospitals.”
Several aspiring Physicians have expressed concerns following the assault on the female doctor at Thiruvananthapuram Government Medical College last week. The attacked female Doctor is quoted to have told Dr. Sulphi N, the Indian Medical Association state president, that she was shocked and regretted her decision to pursue a career as a Doctor and even as a neurosurgeon.
“Despite the noble intentions to save lives and prevent pain and suffering among the patients, Doctors and Medical Professionals continue to put their own lives on the line in the course of their jobs, it is shocking that face such attacks from the very people they are trying to help,” Dr. Sujeeth Punnam, Chair, Alumni Committee of AAPI added.
Dr. Raghu Lolabhattu, Vice Chair, AAPI BOT said, “AAPI urges the Government of India and the State Governments across the country to bring to justice those behind the cruel attacks on the physicians who have dedicated lives for serving the sick, especially during the critical Covid pandemic, risking his own life and that of his dear ones.”
“We at AAPI, the largest ethnic medical organization in the United States urge the Government of India and every state in India to make all the efforts needed to prevent violence against medical professionals and enable them to continue to serve the country with dignity, pride and security. We are shocked by the lack of coherent action against such violence and protect members of this noble fraternity. And we want immediate action against the culprits, who have been carrying on these criminal acts.” For more information on AAPI, please visit: www.aapiusa.org
Forty-six US senators have signed a letter to Senate leaders Charles Schumer, D-N.Y., and Mitch McConnell, R- Ky., expressing serious concerns regarding the stability of Medicare payments for physicians and support for bipartisan, long-term payment reform. The “dear colleague” letter, led by Michigan Democratic Sen. Debbie Stabenow and Wyoming Republican Sen. John Barrasso, also urges Congress to address the budget-neutrality cuts scheduled to take effect in next year’s Medicare physician payment schedule.
The letter comes on the heels of the release earlier this week of the 2023 Medicare physician payment schedule, which has put “Congress on notice that a nearly 4.5% across-the-board reduction in payment rates is an ominous reality unless lawmakers act before Jan. 1,” according to American Medical association (AMA) President Jack Resneck Jr., MD.
In a statement posted on the AMA website, it stated, although the senators’ letter does not address all of the immediate concerns that doctors nationwide have regarding Medicare physician payment, the AMA welcomed the letter as a sign that pressure is building in the Senate to take the actions needed to protect older adults’ access to physician care.
End the statutory annual freeze and provide a Medicare Economic Index update for the coming year.
Extend the 5% Advanced Alternative Payment Model participation incentive and halt the impossible-to-meet revenue threshold increase for five years to encourage more physicians to transition from fee-for-service into alternative payment models.
Waive the 4% pay-as-you-go (PAYGO) sequester triggered by passage of the American Rescue Plan Act.
The AMA offered detailed comments on the proposed 2023 payment schedule.
Picture : TheUNN
“It was immediately apparent that the 2023 Medicare physician payment rates not only failed to account for inflation in practice costs and COVID-related challenges to practice sustainability but also included the damaging across-the-board reduction,” Dr. Resneck noted. “Unless Congress acts by the end of the year, physician Medicare payments are planned to be cut by nearly 8.5% in 2023—partly from the 4% PAYGO sequester—which would severely impede patient access to care due to the forced closure of physician practices and put further strain on those that remained open during the pandemic.”
In their letter, 46 senators agreed that “Congress must address these vital payment challenges before the end of 2022 to ensure seniors continue to have access to care through a wide network” of physicians and other health professionals.
Senate leaders should work with members of Congress “on a bipartisan basis to address” the physician payment cuts that are imminent. “Going forward,” the letter says, “we support bipartisan, long-term payment reforms to Medicare in a fiscally responsible manner.”
Keep doctors’ doors open
Doctors and other health professionals “across the country are facing significant financial hardship due to higher practice costs and the impacts of COVID-19,” the senators’ letter to Schumer and McConnell notes. “Financial uncertainty due to pending payment cuts will only compound these challenges.”
Action should be taken “in the coming weeks” to ensure that doctors and other health professionals “have the resources they need to keep their doors open for seniors and families,” the letter says.
The AMA strongly supports H.R. 8800, the “Supporting Medicare Providers Act of 2022.” The bipartisan legislation aims to stop the scheduled 4.42% cuts to the Medicare physician pay rate and was introduced by Reps. Ami Bera, MD, a Democrat from California, and Larry Bucshon, MD, an Indiana Republican.
“Failure to act in the coming weeks could result in reduced staffing levels and office closures, jeopardizing patient access to care,” the senators noted. “We are especially concerned about this impact in rural and underserved communities. Failure to act on longer-term reforms will undermine Medicare’s ability to deliver on its promises to future seniors and generations.”
The AMA—in collaboration with 120 other physician and health care organizations—has outlined the essential principles (PDF) that can put the nation’s health care system on sustainable financial ground.
A family was shopping at Sam’s Club. Father and mother and their two children of six and two years. A man who never saw this family followed them. He assumed that they came from China. He found a steak knife somewhere in the store. He approached the father and made a cut on the father’s face before disappearing from the store. A little while later, he returned to Sam’s Club with another sharp knife from outside. He then located the young family and then started attacking the two children who were sitting the basket at the front of the shopping cart. The six-year-old child was cut on the face. Before he could do anything further, the people around blocked him and handed him to the police. He confessed to the police that the family came from China and that they were careers of COVID virus. He also confessed that his intention was to kill the six-year-old child. The incident took place on March 14, 2020.
Picture : TheUNN
On October 3rd, the police arrested a thirty-seven-year-old man for assaulting and robbing fourteen women between the ages of fifty and seventy-two. The incidents occurred within two months. All the victims were wearing saris or other Indian clothes. In one incident, a husband and wife who were walking along the road were approached by the man and asked for directions. He then walked behind the couple and pushed the woman to the ground. He then turned to the husband and punched his face. Before running away, he snatched the woman’s necklace. The woman suffered a broken wrist and husband a fractured nose. Police say the attacks were motivated by communal hatred.
This past April, the New York Times reported that Sikhs were physically assaulted three times on the same block in a quiet part of Queens, New York.
Thousands of incidents of discrimination on the basis of color, class, race and heritage have been reported. From March 2020 to March 2022, more than 11400 anti-Asian hate related incidents have been tracked by Coalition for Asian American Pacific Islanders. There is no statistics of the unreported actual incidents. These incidents not only destroy the lives of the victims but also traumatize and disrupt their families and relatives. They are creating fear, suspicion and conflict in the community they belong to. It makes you feel out of place in society. Many feel marginalized. The right of the victimized individuals, of their loved ones and of the people in the community they belong to boldly, freely and safely go out is eroding.
Since the beginning of immigration, Asian Americans have been subject to struggles for equality, social inclusion, and recognition. Suspicion, fear and loathing of strangers, which Asians have been experiencing from time to time, have reached a peak in recent years, especially with the onset of the Covid-19 pandemic. Discrimination through words, behavior, and pretending to be invisible is common, as is physical and psychological abuse. Hate killing is on the rise in our society.
Picture : TheUNN
Such incidents of xenophobia and intolerance, which are so frequent as to damage the values and integrity of the community itself, should be seen as a call for concerted and strong efforts by the affected Asian American communities. Many of those who witness heinous violence and discrimination want to help or stop the victims, but are rendered helpless by their own insecurities. Hate violence doesn’t happen at a specific place or time. The trend suggests that we are all increasingly vulnerable to discrimination and hatred. As with the possibility of witnessing events.
US Census Bureau and US Department of Labor group Chinese, Indians, Filipinos, Pakistan and people from other South and South East Asian countries, and people from the Pacific Islands are counted as a single racial group. This demographic group, known as Asian American Pacific Islanders, is led by Chinese (5.1 million), Indians (4.5 million) and Filipinos (4.1), according to the last count. In New York state, the Asian Pacific Islander community of 2.5 million is considered the fastest growing community in the state.
Asians are seen as a model minority because of the community’s perceived higher degree of socioeconomic success than the other communities. The ironic truth is that this cosmetic stereotype blankets the underserved struggling individuals and families in the community.
Coalition of Asian American Children and Families is a collaborative organization that advocates for social equity and justice and equal rights for educational opportunities for families and children. The Indian Nurses Association of New York (INANI), the voice of Indian nurses in New York state, is partnering with this organization to address anti-Asian hate. It is currently engaged, among other goals, in raising awareness in the community and equip individuals with skills to prevent violence without compromising their own safety.
The strategy, known as Bystander intervention uses 5D methods to develop the awareness, skills and courage needed to intervene in a situation when another individual is in need of help. INANY intends to use community forums and small groups as appropriate platforms and fulfills its mission through them. Dr. Anna George, an associate professor at Molloy University and president of INANY noted that ECHO for Help, a prominent volunteer and charity organization based in Long Island offered the first forum for INANY to provide the training. Dr. Anna George and Dr. Ani Jacob, a Nurse Scientist at Northwell Health System presented for the first time at the ECHO for Help.
Dr. George expressed her gratitude Sabu Lukos and Raju Abraham of ECHO for their unconditional welcome and support for making unity and acceptance a path to compassion. The next presentation against anti-Asian hatred will be at INANY’s general body meeting on November 19 at Dilbar Restaurant in Floral Park in Queens, Dr. George indicated. America’s first Indian Acute Care Nurse Practitioner and Director of New York City Health and Hospitals Corporation Dr. Solymol Kuruvila and Paul D Panakal will be speaking on the 19th of November.
A toddler is thriving after doctors in the U.S. and Canada used a novel technique to treat her before she was born for a rare genetic disease that caused the deaths of two of her sisters.
Ayla Bashir, a 16-month-old from Ottawa, Ontario, is the first child treated as fetus for Pompe disease, an inherited and often fatal disorder in which the body fails to make some or all of a crucial protein.
Today, she’s an active, happy girl who has met her developmental milestones, according to her father, Zahid Bashir and mother, Sobia Qureshi.
“She’s just a regular little 1½-year-old who keeps us on our toes,” Bashir said. The couple previously lost two daughters, Zara, 2½, and Sara, 8 months, to the disease. A third pregnancy was terminated because of the disorder.
In a case study published Wednesday in the New England Journal of Medicine, doctors describe an international collaboration during the COVID-19 pandemic that led to the treatment that may have saved Ayla’s life – and expanded the field of potential fetal therapies. The outlook for Ayla is promising but uncertain.
“It holds a glimmer of hope for being able to treat them in utero instead of waiting until damage is already well-established,” said Dr. Karen Fung-Kee-Fung, a maternal-fetal medicine specialist at The Ottawa Hospital who gave the treatment and delivered Ayla.
Fung-Kee-Fung was following a new treatment plan developed by Dr. Tippi MacKenzie, a pediatric surgeon and co-director of the Center for Maternal-Fetal Precision Medicine at the University of California, San Francisco, who shared her research after the pandemic prevented Ayla’s mother from traveling for care. “We were all motivated to make this happen for this family,” MacKenzie said.
Doctors have treated fetuses before birth for three decades, often with surgeries to repair birth defects such as spina bifida. And they’ve given blood transfusions to fetuses through the umbilical cord, but not medicines. In this case, the crucial enzymes were delivered through a needle inserted through the mother’s abdomen and guided into a vein in the umbilical cord. Ayla received six biweekly infusions that started at about 24 weeks of gestation.
“The innovation here wasn’t the drug and it wasn’t accessing the fetal circulation,” said Dr. Pranesh Chakraborty, a metabolic geneticist at Childrens Hospital of Eastern Ontario, who has cared for Ayla’s family for years. “The innovation was treating earlier and treating while still in utero.”
The unusual partnership also involved experts at Duke University in Durham, N.C., which has led research on Pompe disease, and University of Washington in Seattle.
Babies with Pompe disease are often treated soon after birth with replacement enzymes to slow devastating effects of the condition, which affects fewer than 1 in 100,000 newborns. It is caused by mutations in a gene that makes an enzyme that breaks down glycogen, or stored sugar, in cells. When that enzyme is reduced or eliminated, glycogen builds up dangerously throughout the body.
Picture : Health News,Florida
In addition, the most severely affected babies, including Ayla, have an immune condition in which their bodies block the infused enzymes, eventually stopping the therapy from working. The hope is that Ayla’s early treatment will reduce the severity of that immune response.
Babies with Pompe disease have trouble feeding, muscle weakness, floppiness and, often, grossly enlarged hearts. Untreated, most die from heart or breathing problems in the first year of life.
In late 2020, Bashir and Qureshi had learned they were expecting Ayla and that prenatal tests showed she, too, had Pompe disease.
“It was very, very scary,” recalled Qureshi. In addition to the girls who died, the couple have a son, Hamza, 13, and a daughter, Maha, 5, who are not affected.
Both parents carry a recessive gene for Pompe disease, which means there’s a 1 in 4 chance that a baby will inherit the condition. Bashir said their decision to proceed with additional pregnancies was guided by their Muslim faith.
“We believe that what will come our way is part of what’s meant or destined for us,” he said. They have no plans for more children, they said.
Chakraborty had learned of MacKenzie’s early stage trial to test the enzyme therapy and thought early treatment might be a solution for the family.
The treatment could be “potentially very significant,” said Dr. Brendan Lanpher, a medical geneticist at the Mayo Clinic in Rochester, Minn., who was not involved in the research.
“This is a progressive disease that builds up over time, so every day a fetus or baby has it, they’re accumulating more of the material that affects muscle cells.”
Still, it’s too early to know whether the protocol will become accepted treatment, said Dr. Christina Lam, interim medical director of biochemical genetics at the University of Washington and Seattle Children’s Hospital in Seattle.
“It’s going to take some time to really be able to establish the evidence to definitively show that the outcomes are better,” she said.
Your time is precious — and limited. So when it comes to working out, it’s not uncommon to wonder: what exercise burns the most calories?
Exercise scientists have rigorously studied the amount of energy people expend during different types of exercise, and they’ve determined which workouts are best for burning calories. The thing to keep in mind: the more muscles you engage and the harder (and longer) you push those muscles, the more energy your body will churn through, says Dr. Tim Church, an exercise researcher and a professor of preventative medicine at Pennington Biomedical Research Center at Louisiana State University. So in order to maximize the number of calories you’ll burn, “you want an exercise that uses both lower and upper body muscle groups and is performed at a high intensity,” Church says.
Picture : Stylist
A study on one popular CrossFit workout called the “Cindy” — in which a person does a series of pull-ups, push-ups and squats in as many rounds as possible — found that it burned an average of 13 calories per minute. The workout lasts 20 minutes, so exercisers burned an average of 260 calories in total. While perfect apples-to-apples studies aren’t available, some Tabata research has shown that one of these workouts — composed of 4-minute training blocks that mix maximum-intensity bouts of resistance and aerobic training with short periods of rest — burns 14.5 calories per minute, or 280 calories during a 20-minute workout.
These per-minute calorie averages beat out many traditional forms of exercise. “But there’s such a variety within these classes and the people doing them that scores are all over the map,” says John Porcari, author of the Tabata study and a professor of exercise and sports science at the University of Wisconsin, La Crosse. For example, some people in his Tabata study burned up to 360 calories during the 20-minute workout, or 18 calories per minute.
Yet “per-minute” calorie burn isn’t always the best way to assess a workout’s energy demands, Porcari says. The total time spent training and a person’s willingness to stick with a workout are also important factors. “You can crank like the dickens for 30 seconds and burn a lot of calories,” he says. So if you’re extremely short on time, high-intensity interval training (HIIT) is probably your best option. But in the real world, Porcari says, many people won’t be comfortable (or capable of) engaging in regular or extended bouts of high-intensity training.
He says a “more fair” way to assess an exercise’s true energy demands is to ask people to do it at a pace that is comfortable for them. And when it comes to vigorous, calorie-burning exercises that people are comfortable doing for extended periods of time, running usually comes out on top. “When you look at the literature, running tends to burn more calories than other modalities,” he says.
According to an online calorie estimator from the American Council on Exercise, a 115-pound person running for 30 minutes at a slow-to-moderate pace (a 10-minute mile) would burn about 260 calories: the same amount people who did CrossFit typically torched in 20 minutes, according to the research. A 175-pound person would burn nearly 400 calories during that same 30-minute run. Pick up the pace, and you can achieve an even greater rate of calorie burn.
You may be wondering whether more intense forms of exercise lead to a higher rate of calorie expenditure even after training is finished — or a so-called “afterburn effect.” Research from Colorado State University has shown that, yes, intense exercise does keep a person’s metabolism humming longer than mild exercise. But this afterburn effect tends to peter out quickly — within a few hours — and it accounts for a small fraction of the total calories a person expends during and after exercise.
Also, a workout’s length — not just its intensity — helps to keep a person’s metabolism elevated after training, finds a review from the University of New Mexico. So if your goal is to burn the maximum amount of energy, you’ll want to find an exercise that is vigorous and that you can stick with for a long stretch of time.
For a lot of people, that mode is running. For others, it may be fast stationary cycling or Tabata or using an elliptical. The research suggests all are more or less comparable if you’re able to put in the time and keep up the intensity.
The bottom line? The best workout for burning calories is “the one you actually do,” Church says. You can find extreme forms of exercise that maximize per-minute calorie burn. But if you don’t stick with them or do them regularly, they’re not much good to you.
Mindfulness meditation worked as well as a standard drug for treating anxiety in the first head-to-head comparison.
The study tested a widely used mindfulness program that includes 2 1/2 hours of classes weekly and 45 minutes of daily practice at home. Participants were randomly assigned to the program or daily use of a generic drug sold under the brand name Lexapro for depression and anxiety.
After two months, anxiety as measured on a severity scale declined by about 30% in both groups and continued to decrease during the following four months.
Study results, published Wednesday in the journal JAMA Psychiatry, are timely. In September, an influential U.S. health task force recommended routine anxiety screening for adults, and numerous reports suggest global anxiety rates have increased recently, related to worries over the pandemic, political and racial unrest, climate change and financial uncertainties.
Picture : ABC News
Anxiety disorders include social anxiety, generalized anxiety, and panic attacks. Affected people are troubled by persistent and intrusive worries that interfere with their lives and relationships. In the U.S., anxiety disorders affect 40% of U.S. women at some point in their lives and more than 1 in 4 men, according to data cited in U.S. Preventive Services Task Force screening recommendations.
Mindfulness is a form of meditation that emphasizes focusing only on what’s happening at the moment and dismissing intrusive thoughts. Sessions often start with breathing exercises. Next might be “body scans” — thinking about each body part systematically, head to toe. When worried thoughts intrude, participants learn to briefly acknowledge them but then dismiss them.
Instead of ruminating over the troubling thought, “you say, ‘I’m having this thought, let that go for now,’’’ said lead author Elizabeth Hoge, director of Georgetown University’s Anxiety Disorders Research Program. With practice, “It changes the relationship people have with their own thoughts when not meditating.”
Previous studies have shown mindfulness works better than no treatment or at least as well as education or more formal behavior therapy in reducing anxiety, depression and other mental woes. But this is the first study to test it against a psychiatric drug, Hoge said, and the results could make insurers more likely to cover costs, which can run $300 to $500 for an 8-week session.
The results were based on about 200 adults who completed the six-month study at medical centers in Washington, Boston and New York. Researchers used a psychiatric scale of 1 to 7, with the top number reflecting severe anxiety. The average score was about 4.5 for participants before starting treatment. It dropped to about 3 after two months, then dipped slightly in both groups at three months and six months. Hoge said the change was clinically meaningful, resulting in noticeable improvement in symptoms.
Ten patients on the drug dropped out because of troublesome side effects possibly related to treatment, which included insomnia, nausea and fatigue. There were no dropouts for that reason in the mindfulness group, although 13 patients reported increased anxiety.
Dr. Scott Krakower, a psychiatrist at Zucker Hillside Hospital in New York, said mindfulness treatments often work best for mildly anxious patients. He prescribes them with medication for patients with more severe anxiety.
He noted that many people feel they don’t have time for mindfulness meditation, especially in-person sessions like those studied. Whether similar results would be found with online training or phone apps is unknown, said Krakower, who was not involved in the study.
Olga Cannistraro, a freelance writer in Keene, New Hampshire, participated in an earlier mindfulness study led by Hoge and says it taught her “to intervene in my own state of mind.’’
During a session, just acknowledging that she was feeling tension anywhere in her body helped calm her, she said.
Cannistraro, 52, has generalized anxiety disorder and has never taken medication for it. She was a single mom working in sales during that earlier study—circumstances that made life particularly stressful, she said. She has since married, switched jobs, and feels less anxious though still uses mindfulness techniques.
Ayurveda, the science of life has brought true health and wellness to millions of individuals throughout the ages with simple changes in daily living practices.
This ancient art of healing has been practiced continuously for over 5,000 years. Ayurvedic practices restore the balance and harmony of the individual, resulting in self-healing, good health and longevity. Incorporating just a few of these proven methods into your lifestyle can bring about radical changes in your life.
The principles of many natural healing systems now familiar in the West, such as Homeopathy and Polarity Therapy, have their roots in Ayurveda. The understanding that we are all unique individuals enables Ayurveda to address not only specific health concerns but also offers explanation as to why one person responds differently th an another.
Ayurveda uses herbs and spices like basil, turmeric, garlic, ginger and aloe vera, as well as yoga exercises, to treat physical and psychological problems.
Interest in Ayurveda in the United States began in the 1970’s, largely as the result of efforts by the Maharishi Mahesh Yogi organization of Transcendental Meditation. Interest continued to grow as Indian physicians came to the United States in the 1980’s. Among these physicians were Dr. Vasant Lad, Dr. Sunil Joshi and Dr. B.D. Triguna.
In the late 1980’s Dr. Deepak Chopra wrote “Perfect Health”, his famous introductory book on Ayurveda for the general public. This opened the door of India ‘s ancient healing science for many Westerners. Furthermore, several American pioneers helped attract attention to Ayurveda and influence its growth.
Picture: FB
They include Dr. David Frawley, of the American Institute of Vedic Studies, and Dr. Robert Svoboda, a Westerner who completed India ‘s BAMS program. As interest and awareness grew, training programs of various degrees emerged. In 1995, the California College of Ayurveda was founded and was the first State-approved practitioner training program in the United States .
The National Ayurvedic Medical Association is the major body in the United States representing the Ayurvedic profession. A non-profit association, it was founded in 1998 by four individuals: Dr. Marc Halpern, of the California College of Ayurveda, Wynn Werner, of the Ayurvedic Institute, Kumar Batra, and Cynthia Copple. Indians trained Ayurvedic physicians who come to the United States on a work visa or through immigration may practice Ayurveda within a allowable scope.
The interest in Ayurveda has grown steadilynin the past few decades, and many more people from across the world are seeking Ayurveda treatment in India and in the many facilities where they are being ofered. For too many, who have been “given up” by the Western medicine, the first choice of treatment, Ayurveda offers an “alternate” and several hundreds seek and find solutiomns to their physical and mental illnesses.
In December 2000, I was diagnosed with Uveitis with Vasculitis and peripheral neovascularization. After being treated with Prednisone, a steroid, upto 100 mg per day, though my vision had improved, it had inflicted several side-effects on my entire physical as well as mental health.
Later on, after several surgeries that included a cataract, laser-surgeries, and Vitrectomy, I decided to seek ayurvedic treatment at Sreedhareeyam Ayureda Gaveshana Kendram, an endeavor by Nellikattu Mana, a Namboodiri family with traditional experiences and talents in Ayurveda treatment especially in the treatment of eye diseases.
After undergoing a full three weeks of treatment for four times in two years at Sreedhareeyam, my vision had showed signs of improvement. The inflammation on the retina was substantially reduced and the damage to the optic nerve was contained, which I thought, was the biggest achievement of the treatment I received at Sreedhareeyam. The cataract on my left eye was healed without a surgery, although the pressure on my right remained elevated. Medical Superintendent at Sreedhareeyam, Dr. N P P Namboothiri, a famous eye physician and the mentor and guide to the hospital, helped me “restore” my vision. .
Picture: Sreedhareeyam
At Sreedhareeyam, where more than two dozen trained eye-specialists with degrees in Medicine, the primary focus has been on Ayurvedic treatments for all types of diseases.
However, specialized treatments are given for the various diseases affecting the positions above the neck. Most of the eye diseases, which have got no treatment in modern medicine, have been successfully treated here. People come here from all strata of society and from all corners of the world.
Most of the patients here at this nearly 200-bed hospital are those who have tried the regular Western medicines and have been given up as having no cure for their problems. Just like me, most of them choose to come here as the final resort, and hope that Sreedhareeyam is the answer to many of their eye diseases.
Aravind Kumar, a college student in Delaware, told this writer, “I was born with congenital cataracts in both eyes.” After six major eye operations that included surgeries to remove cataract as well as intra-ocular-lens implantation, he was was left with limited eyesight of about sixteen inches. “It was during the summer of 2003 that we made our first visit to India in several years, when we learned more about Ayurveda treatments specific to eyes and vision at Sreedhareeyam,” Aravinf recalls.
In November of 2004, his first ever treatments began. “A few days into the treatment, my first eye refraction exam was done. From five feet I was able to see three lines of text clearly. After ten more days a second eye refraction was done. This time, from six feet I could read almost five lines of text. I was amazed that, through Ayurveda and Sreedhareeyam, I was able to see more things far away,” this young boy from Allen Ttown, PA narrates. “My local Ophthalmologist in the US, who is renowned in the field of ophthalmology, was amazed to see the improvement in my vision.”
Restoring vision from birth defects is not a quick-fix. It takes time. Since 2004, he had gone back to Sreedhareeyam for five courses of treatments, each for a period of three to four weeks. “During each visit I have undergone treatments like Nasyam, Netra Dhara, Sirodhara, Pothichil, Tharpanam, etc.,” said Aravind, who went to Sreedhareeyam in Janauary 2008 for yet another phase of his treatment.
“I am experiencing dramatic results. Prior to the treatment, my peripheral vision was very poor and I had a tough time focusing. Now my peripheral vision is much better and I’m able to focus better. This has helped me immensely in my school work and day-to-day life. My astigmatism has been reduced, I am able to concentrate more than I used to and I can see things a little bit farther than I used to. My visits also gave me an opportunity to meet and talk to several visually under-previleged from across the globe, who come there with the hope for better vision. Most of them being tried and rejected by modern medicine.” Aravind tesxtifies, “Sreedhareeyam is truly the Ayurvedic hospital and they definitely live up to their motto of “vision for all”
Jayachandran, a 43-year-old male, originally from Bangalore, now living in Japan, told this writer, “I was diagnosed with Retinitis Pigmentosa, a rare hereditary disorder, which causes poor night vision and ever-narrowing field of vision beginning in childhood.”
About 12 years ago, he lost his vision completely and was declared blind. After being treated around the world for several years with no positive results, he heard about Sreedhareeyam, and came here about two years ago. “It’s my fifth visit in two years. I am beginning to see for the first time in 12 years,” Jayachandran said with a sense of joy and satisfaction. “The doctors here have been able to arrest the process of degeneration, and they have assured me that I can regain about 10 to 20 percent of my vision, which is great.”
Simran, 10 and Sonal, 12, two sisters from Sydney, Australia, were here for treatment for Retinitis Pigmentosa. Online search for treatment for this rare eye disease by their desperate parents brought them here at Sreedhareeyam. After four visits with a gap of three months between each visit, now the doctors at Sreedhareeyam have advised them to return to Sreedhareeyam after two years.
There was a sense of relief and inner joy on the face of the Mr. V. Goyal, the father of these two young kids, realizing that the process of degeneration has been arrested and their vision will be stable.
Ella Murugan is a 20-year-old boy from Salem, Tamil Nadu. He was diagnosed with Retinal Detachment, and was treated at the famous Sankara Netralaya in Chennai for more than three years. “After each surgery done on my eyes at Sankara Nethralaya, I began to lose my vision, and I became totally blind,” he said. “This is my fourth visit in less than two years, and now my eyes can see things and people around me, as though they are shadows.” He expressed confidence that in the near future, he will begin to see more clearly.
The story of Abdul, a 10-year-old boy from northern Kerala was heart-breaking. While playing with his friends, a sharp wooden stick pierced through his right eye, severely damaging his retina and the optic nerves, resulting in severe bleeding of the retina, thus leading to the loss of vision.
In December 2005, he was at Sreedhareeyam for his third hospitalization in 15 months. “Also, his bleeding on the retina has been contained,” his mother told this writer. “He has begun to see partially,” she added.
These are only a few of the hundreds of success stories one gets to witness during the stay from patients who come here for various eye diseases. “Results from the treatment here are the only publicity we do,” said, Narendran, Executive Director of Sreedhareeyam. “Our ever-increasing number of patients is a witness to the impact of the treatment patients receive here. Our publicity is by word-of-mouth only of these success stories.”
There have been a number of instances at Sreedhareeyam where success was found while it was only failure that the patients met with in other systems of medicine. According to Dr. N P P Namboodiri, its all miracles in the sense that all these helped manifest the capabilities of Ayurveda in an area of health care that needs specialization. A large number of such cases from the long history of the hospital stand testimony to the supremacy of Ayurveda system of medicine over other systems in treatment of eye diseases.
“At Sreedhareeyam, ours is a humble attempt to treat the disease and annihilate it through the way of nature,” says Dr. Narayanan Namboothiri, who treats patients from the same room in Naalukettu, where he was born. “Patients from all over the world come here for various eye diseases, including those suffering from Cataract, Glaucoma, Macular Degeneration, and Diabetic Retinopathy. We strive to give them our best, trusting in God’s power to heal them,” the gentle-speaking Dr. Narayanan Namboothiri says.
“At Sreedhareeyam, we strive to maintain and cultivate the hospital into a shrine of hope for hundreds of people who seeks cure from their various and mysterious ailments.
Fortunately, due to our long history of successes, we have an astounding number of patients coming in daily from the length and breadth of the country, seeking cure,” Dr. Namboodiri says.
“In the field of the treatment of eye diseases, we desire to rank ourselves from an international perspective. The history of the miraculous cures at Sreedhareeyam and our eminent panel of doctors proclaim our supremacy in this field. With all our expertise and resources, we foresee a wider dimension for our services to the society in the future,” the physician says with a sense of pride and hope. In the wake of the prevailing situation, Sreedhareeyam, according to Dr. Namboothiri, “aspires for a wider participation on a large scale in the battle to annihilate darkness of human eye from the face of earth.
All the treatments offered here are unique in the sense that the medicines used for all these treatments are produced at the Manufacturing Unit of the hospital. “The ingredients of the medicine as well as the treatment procedures are all according to those parchments (‘thaliyolas’) and ancient books (‘grandhas’), which counts among the traditional and precious assets owned by the Mana,” Dr. Narayanan Namboothiri, the young and dynamic physician, who heads the research unit of the hospital, says.
The research centre is studying several manuscripts on ayurveda, found all over the State and putting them in order. Medicines are grown in the Koothattukulam campus, where the ancestral home of the vaidyas. Medicines are also manufactured here under the supervision of Narayanan Namboothiri, the Chief Medical Officer of the hospital.
Experts predict that hundreds of herbs used for centuries by traditional healers in India could soon be on western pharmacy shelves. With 15,000 plant species, India is well placed to increase its share of the $75billion global market in medicinal plants, which is growing by at least 7% a year.
The Indian Council of Medical Research has launched a series of studies to test the health claims surrounding a variety traditional medicines. Clinical trials have shown that herbal remedies for asthma, diabetes and even sexually transmitted diseases may be effective. The council is looking at treatments for a range of other conditions used for over a thousand years by practitioners of Ayurveda and Siddha medicine.
Professor Ranjit Roy Chaudhury, a member of the council, said that in some cases the herbs may be more effective than Western-style medicines. “We have plants for bronchial asthma, hepatitis and arthritis,” he said. “We have other plants which have been shown to be effective for treating sexually transmitted diseases and they have been used in that way by tribal populations for centuries. We have herbs where you can relieve headache, fever, gastroenteritis, sneezing and coughing. These conditions can easily be alleviated.”
Professor Chaudhury acknowledged that in some cases the council will be unable to prove that the herbs work. This is because many of the remedies are based on a combination of plants which taken on their own would not be effective. “There are hundreds of herbs but we are unable at the moment to do very good testing for combinations of plants. “In the Ayurvedic system they use usually combinations. But testing combinations with modern technology is difficult.”
The world as a whole is switching over from chemical drugs to natural drugs because they are non-narcotic, they have no side-effects and are easily available. The world is interested in simpler and gentler therapies – especially for ageing, the problem of obesity, diabetes, neurological disorders, cardiac diseases and digestive problems.
Even as the ancient ayurveda science is becoming increasingly popular, it has encountered several hurdles too. Lack of funding for research has limited its growth and wider use. However, utilizing the available on going research, basing them on the ancient wisdom of the Rishis and Munis, and availing the few encouraging measures from the government of India,
The Ayurvedic profession is growing steadily in the United States of America, just as is in and around the world. Educational institutions are becoming more established and the Associations are working to give the profession a voice and address regulation issues. Ayurveda is likely to continue to grow in America and take its place among the other licensed health care professions.
GHS and Pre-GHS/CME Family Tour to Vietnam, Cambodia and Kuala Lumpur Registration is Open and Filling up fast
Chicago, IL, November 8th, 2022 : “The registration for AAPI’s 16th annual Global Healthcare Summit 2023 at the at the prestigious Novotel Visakhapatnam Varun Beach, Andhra Pradesh, India from January 6th to 8th, 2022 and the Pre-GHS/CME tour to exotic destinations, Vietnam, Cambodia and Kuala Lumpur is filling up fast,” Dr. Ravi Kolli, President of the American Association of Physicians of Indian Origin (AAPI) announced here today. “Physicians and healthcare professionals from across the country and internationally will meet and participate in the scholarly exchange of medical advances, to develop health policy agendas, and to encourage legislative priorities in the coming year. We look forward to seeing you in Visakhapatnam!” said Dr. Ravi Kolli
The GHS 2023 by AAPI is being organized in collaboration with Andhra Medical College Alumni Association, Andhra Medical College, Indian Medical Association, AP, Association of Telugu Medical Graduates in the USA and Rangaraya Medical College Alumni Association and the Government of the State of Andhra Pradesh.
While elaborating on the themes and areas that are going to be covered during the Summit, Dr. V. Ranga, Chair of AAPI BOT, says, “The GHS 2023 will focus on Mental Health and Physician Burnout, Rural Health Initiatives, Infant and Maternal Health issues as well as Medical Jeopardy, Research Poster presentations by medical students.”
Picture: TheUNN
Dr. Prasad Chalasani, Chair of AAPI GHS-USA says, “With hundreds of physicians from the United States, the Summit is expected to be attended by nearly 400 delegates from around the world. AAPI Global Healthcare Summit (GHS) will have many new initiatives and also will be carrying the torch of ongoing projects undertaken by AAPI’s past leaders.”
Many of the physicians who will attend this convention have excelled in different specialties and subspecialties and occupy high positions as faculty members of medical schools, heads of departments, and executives of hospitals and pharma companies. “The AAPI GHS offers an opportunity to meet directly with these physicians who are leaders in their fields and play an integral part in the decision-making process regarding new products and services,” Dr. Anajan Sammader, President-Elect of AAPI said.
The preliminary program is in place, the major attractions include 12 hours of cutting-edge CME with renowned speakers, CEO Forum, Innovation Forum, Entrepreneur Forum, Women’s Forum, Product Theaters to highlight the newest advances in patient care and medical technology. Alumni meetings for networking, also an AAPI-India Strategic Engagement Forum to showcase the AAPI initiatives in India, TB Eradication in India and recognition of AAPI Award winners will make this Summit unique,” Dr. Ravi Raju, Chair of GHS-India said.
In addition to offering over 10 hours of cutting-edge CMEs to the physicians, the event will have product theaters/promotional opportunities, plenary sessions, multi-segment CEOs Forum, women’s leadership forum. The convention will be addressed by senior world leaders, including celebrities from the entertainment world, said Dr. Sudhakar Jonnalagadda, Chief Advisor of the GHS 2023.
Picture: TheUNN
Dr. Kolli expressed gratitude to all the Chairs and members of various Committees who are working hard to put together a great Summit and to enable members to return home with memories that will last a life time.
According to CME Chair Dr. Sreeni Gangasani and Academic Chair Dr. Sharma Prabhakar, some of the topics for the CMEs will include Psychiatry, Ophthalmology, Pediatrics, Oncology. “In our efforts to realize the core mission of AAPI, which is to share the best from leading experts from around the world, to collaborate on clinical challenges, the GHS in Visakhapatnam will have clinical tracks that are of vital to healthcare in India,” Dr. Ganagasani said.
Dr. Lokesh Edara and Dr. Brahma Sharma, who are the co-chairs of International medical education will conduct a high-powered panel discussion by International Medical Education experts including CEOs of ECFMG, WFMC, and National Medical Council officials. Dr. B K Kishore, an academic expert will lead discussions on research methodology and scientific writings.
Dr. Sampath Shivangi, AAPI Legislative Committee Chair said, “We are collaborating with senior leaders from leading healthcare organizations including pharmaceuticals, device and medical equipment manufacturers and major medical teaching institutions, hospitals and the Ministries of Health, External/Overseas Affairs and regulatory bodies to attend and coordinate with AAPI with an ultimate goal to providing accessible and affordable high-quality healthcare to all people of India.”
Picture: TheUNN
Dr. Manoj Jain, Chair of CETI – Collaboration to Eliminate TB in India supported by CDC and USAID will discuss their ongoing long-term TB Elimination Projects in India. CEO Forum Chair Dr. Joseph Chalil said, “We will have discussions on Equity, Ethics and Physician Burnout Issues.” The Women’s Forum chair Dr. Udaya Shivangi announced that “there will be meaningful discussions and policy statements on gender bias and its impact on leadership.”
Dr. Satheesh Kathula, Vice President of AAPI, says, “It is these learning opportunities and collaborative relationships that have now enabled AAPI and participating organizations to plan and prepare for an outstanding event that is expected to have over 300 prominent and experienced physicians and surgeons of Indian origin from around the world, who are very passionate about serving their homeland, Mother India.”
Dr. Meher Medavaram, Secretary of AAPI says, “Being organized at this critical phase, especially as the world is emerging out of the Covid pandemic, GHS 2023 is aimed at exploring possibilities for greater collaboration and cooperation between the physicians and health care providers in India with those of Indian origin and major health-care providers abroad.”
“Harnessing the power of Indian Doctors worldwide, the AAPI Global Healthcare Summit platform has evolved with the support of prominent global and Indian medical associations . AAPI’s mission is to make a positive and meaningful impact on the healthcare delivery system both in the US and in India,.” Dr. Sumul Rawal, Treasurer of AAPI pointed out.
Picture: TheUNN
Healthcare in India is one of the largest sectors, in terms of revenue and employment. India is making significant improvements in its healthcare infrastructure and is building modern medical facilities throughout India. Indian doctors have made tremendous progress in the 21st century and India is now being touted as a medical tourism hub. With hundreds of physicians joining from the United States, the summit is expected to be attended by three hundred delegates from around the world. AAPI Global Healthcare Summit (GHS) will have many new initiatives and will be carrying the torch of ongoing projects undertaken by AAPI’s past leaders.
The Global Healthcare Summit has come a long way from the first Indo-US Healthcare Summit launched by AAPI USA in 2007. Since then, AAPI has organized 15 Indo – US/Global Healthcare Summits and developed strategic alliances with various organizations.
AAPI is hopeful that several international healthcare industry partners are looking for opportunities to participate at this event for greater collaboration on Research & Development and philanthropic engagements. Dr. Kolli added.
Representing the interests of the over 120,000 physicians of Indian origin, leaders of American Association of Physicians of Indian Origin (AAPI), the largest ethnic organization of physicians, for 40 years, AAPI Convention has provided a venue for medical education programs and symposia with world renowned physicians on the cutting edge of medicine.
“Physicians and policy makers, legislators and entrepreneurs will brainstorm at the GHS to find meaningful, impactful, actionable plans and solutions to make health care accessible, affordable, and equitable to all segments and regions of the populations, as health and wellness are fundamental and foundational to individuals and societies to progress and development. Healthcare professionals from across the country and internationally will take part in the exchange of knowledge of medical advances and to develop health policy agendas. We look forward to seeing you in Visakhapatnam!” said Dr. Ravi Kolli. For more details, please visit: www.aapiusa.org/ To register for the Global Healthcare Summit 2023, please visit: https://summit.aapiusa.org
Pacemakers are usually given to those who have lived a long life and now their heart needs an extra assistance. For me, I was born with a heart defect,” Shree, 26, wrote.
Indian-American model Shree Saini, who was declared the first runner-up at the Miss World 2021 pageant, recently revealed that she is undergoing heart surgery for a new pacemaker implant as her “current pacemaker batteries have died”. A heart patient, Shree, who got a pacemaker at the age of 12, went on to share that she has to “undergo a total of eight pacemaker replacement surgeries” in her lifetime.
“I would so greatly appreciate your prayers. There will be no visitors allowed at the hospital. I want to thank everyone who has been there for me. For those who may not know, I was born with a complete heart block, where my upper and bottom chambers did not communicate with each other. My block led me to me having a very low heart rate and feel terribly fatigued,” she mentioned in a note on Instagram.
“The pacemaker paces my heart to beat at a normal rate. It does this by using the pacemaker to send electric shocks to my heart which allows it to beat at a normal rate. Average age of a pacemaker recipient is age 80. Pacemakers are usually given to those who have lived a long life and now their heart needs an extra assistance. For me, I was born with a heart defect,” Shree, now 26, penned.
Adding that she is sharing her story to “encourage people to have a greater sense of hope even in their hardships”, she wrote, “Let’s rise up from our challenges with a victor, not a victim mindset.”
Picture: Beauty Pageant
Shree, who was also adjudged Ambassador Beauty With Purpose at the 2021 Miss World, thanked her well-wishers for their constant support. “I still remember being a kid and being so confused, scared while waiting for my initial surgery. I do remember the teachers and peers who were there for me. I will forever be grateful for people who cared, reached out with comforting words and whose love filled me with strength. Thank you for keeping me in your thoughts. I am the sum of God’s blessings, parents’ unconditional love and the blessings of so many people. So grateful for scientists, doctors for creating this remarkable pacemaker technology, that literally allows me to live today!”
About the size of a pocket watch, artificial pacemakers are implanted under the skin through an incision in the chest. The device is connected to the heart through leads or wires that deliver electrical signals that regulate the heart’s activity. “Pacemakers are small machines placed to generate heart beats. When your heart beats slows down to less than 50-60 beats, with or without heart conduction tissue, it indicates damage to your heart’s wiring system, or in cases of heart failure where a patient’s heart do not beat in tandem to produce a good pulse or output, then the doctor recommends these small machines to improve the quality of life, said Dr Bipeenchandra Bhamre, consultant cardiac surgeon, Sir H. N. Reliance Foundation Hospital and Research Centre in Mumbai, adding that ECG and Holter monitoring tests help to determine the need of pacemakers.
According to the expert, two types of machines are widely used — single chamber and dual chamber — depending on the number of heart chambers affected. “Periodic check up, every year, is required to check for battery. Your doctor will recommend the type of machine better for you,” he said.
Dr Pankaj Batra, senior interventional cardiologist, Fortis Escorts Faridabad, told indianexpress.com that the PPI or Permanent Pacemaker Implantation procedure takes about an hour to be completed. “Permanent pacemaker insertion is considered a minimally invasive procedure. Transvenous access to the heart chambers under local anesthesia is the favored technique. It is not a surgery,” said Dr Batra, adding that “in case of congenital heart defects, pacemakers may be preferred for a long life.”
A National Center for Biotechnology Information (NCBI) review also suggested that the primary purpose of such a device is to maintain an adequate heart rate, either because the heart’s natural pacemaker is not fast enough, or there is a block in the heart’s electrical conduction system. “Modern pacemakers are externally programmable and allow the cardiologist to select the optimum pacing modes for patients on a case-to-case basis,” explained Dr Batra and further said that replacement is usually done after 10 to 15 years using a “minor procedure”.
While pacemakers can be temporary in cases of a heart attack, permanent pacemakers are used to control long-term heart issues. “Pacemaker can relieve some arrhythmia symptoms, such as fatigue and fainting. A pacemaker also can help a person who has abnormal heart rhythms resume a more active lifestyle,” mentioned the NCBI review. Agreed Dr Batra and mentioned that pacemakers are needed to “improve the quality of life”, and with minimal heart-related issues. (Courtesy: The Indian Express)

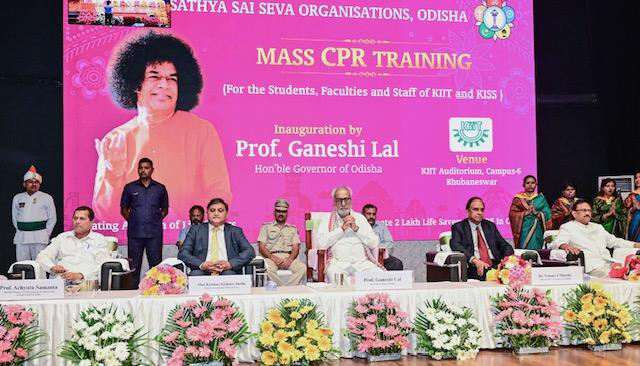

 Addressing the over 1,000 delegates from around the nation, Dr. Ravi Kolli, Immediate past President of AAPI spoke about the origins of AAOI 41 years ago and how the physicians of Indian origin have been sought after for their excellence in Medicine. “I applaud you and thank you for your support all through the year. And your presence here with your blessing and your goodwill and warm wishes for the successful 41st Ave annual convention here in our brother City of Brotherly Love Philadelphia,” Dr. Kolli said.
Addressing the over 1,000 delegates from around the nation, Dr. Ravi Kolli, Immediate past President of AAPI spoke about the origins of AAOI 41 years ago and how the physicians of Indian origin have been sought after for their excellence in Medicine. “I applaud you and thank you for your support all through the year. And your presence here with your blessing and your goodwill and warm wishes for the successful 41st Ave annual convention here in our brother City of Brotherly Love Philadelphia,” Dr. Kolli said.








 The Columbus AAPI Convention team has echoed her sentiments, It said, “We have personally known and worked closely with Dr. Anjana Samadder. She has great leadership qualities which she proved during her tenure as local chapter President (Central Ohio), Regional Director (Ohio and Michigan) and as AAPI National Treasurer. She has also served diligently in different capacities within AAPI including being National Coordinator for AAPI Annual Convention, 2018 in Columbus.
The Columbus AAPI Convention team has echoed her sentiments, It said, “We have personally known and worked closely with Dr. Anjana Samadder. She has great leadership qualities which she proved during her tenure as local chapter President (Central Ohio), Regional Director (Ohio and Michigan) and as AAPI National Treasurer. She has also served diligently in different capacities within AAPI including being National Coordinator for AAPI Annual Convention, 2018 in Columbus. (Philadelphia, PA—July 8th, 2023) The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions was officially inaugurated with the chanting of the Sanskrit Mantras, seeking blessings from above, Ribbon cutting and lighting of the traditional Lamp by AAPI leaders and distinguished guests on July 7th, 2023 at the famous Philadelphia Marriott Downtown in Philadelphia, the birthplace of US Independence.
(Philadelphia, PA—July 8th, 2023) The 41st annual American Association of Physicians of Indian Origin (AAPI) Convention and Scientific Sessions was officially inaugurated with the chanting of the Sanskrit Mantras, seeking blessings from above, Ribbon cutting and lighting of the traditional Lamp by AAPI leaders and distinguished guests on July 7th, 2023 at the famous Philadelphia Marriott Downtown in Philadelphia, the birthplace of US Independence.







 The AAPI Presidential Healthcare Leadership Award 2023 is a well-deserved recognition of Dr. Shaya’s exceptional contributions to the future of healthcare delivery. His visionary approach and commitment to innovation have propelled the industry forward and inspired countless healthcare professionals to embrace new possibilities.
The AAPI Presidential Healthcare Leadership Award 2023 is a well-deserved recognition of Dr. Shaya’s exceptional contributions to the future of healthcare delivery. His visionary approach and commitment to innovation have propelled the industry forward and inspired countless healthcare professionals to embrace new possibilities.
 In his response to being chosen for the award, Dr. Shivangi said, “I am truly honored to receive this prestigious Xavier University of Aruba award, which has made a worldwide impression as a premier Institute of learning. It’s even a greater honor to be in such distinguished ranks of those present and past honorees, who have made important contributions to healthcare.”
In his response to being chosen for the award, Dr. Shivangi said, “I am truly honored to receive this prestigious Xavier University of Aruba award, which has made a worldwide impression as a premier Institute of learning. It’s even a greater honor to be in such distinguished ranks of those present and past honorees, who have made important contributions to healthcare.”
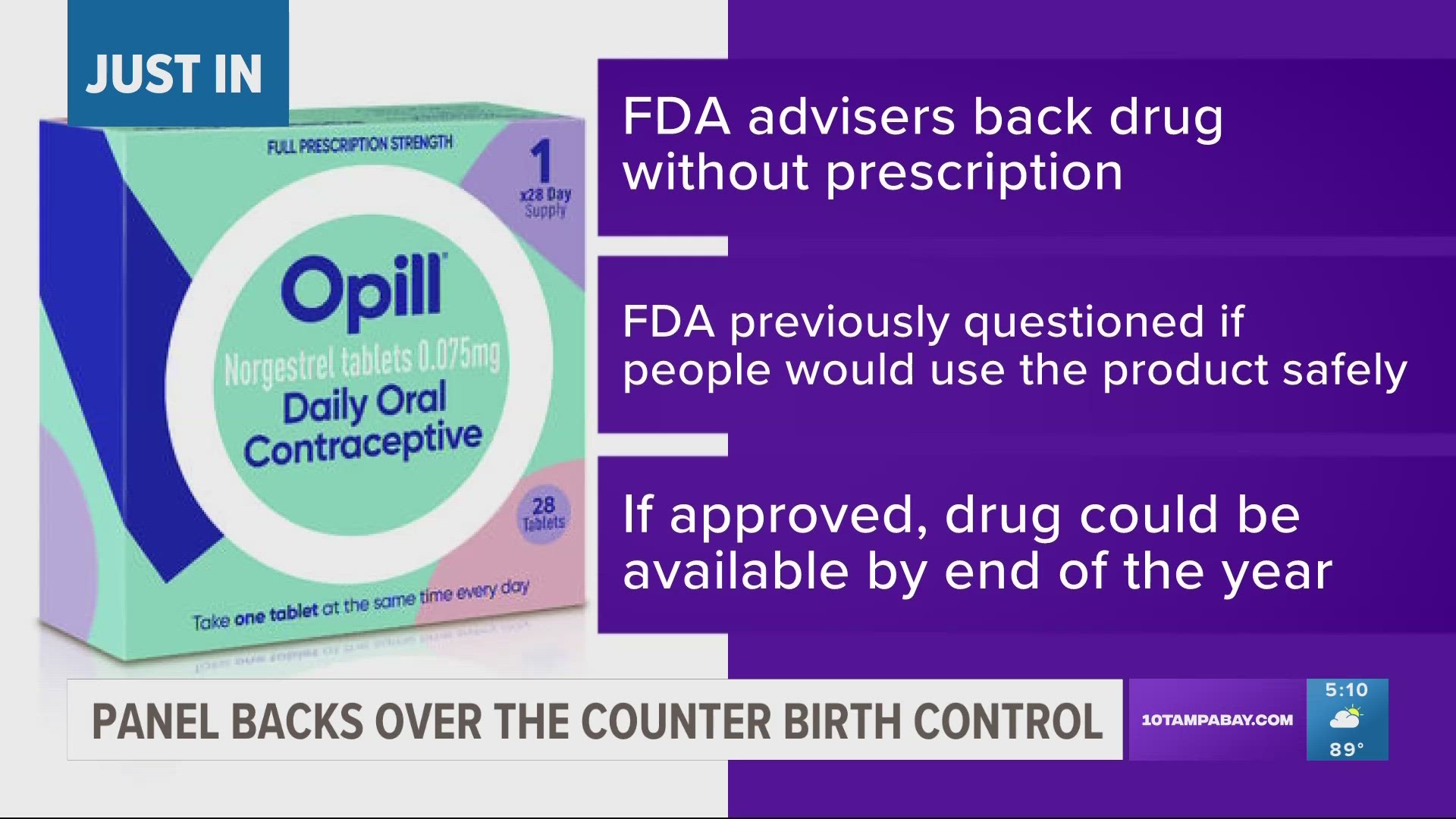
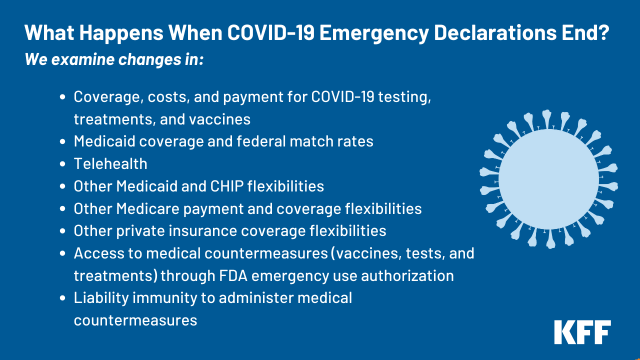





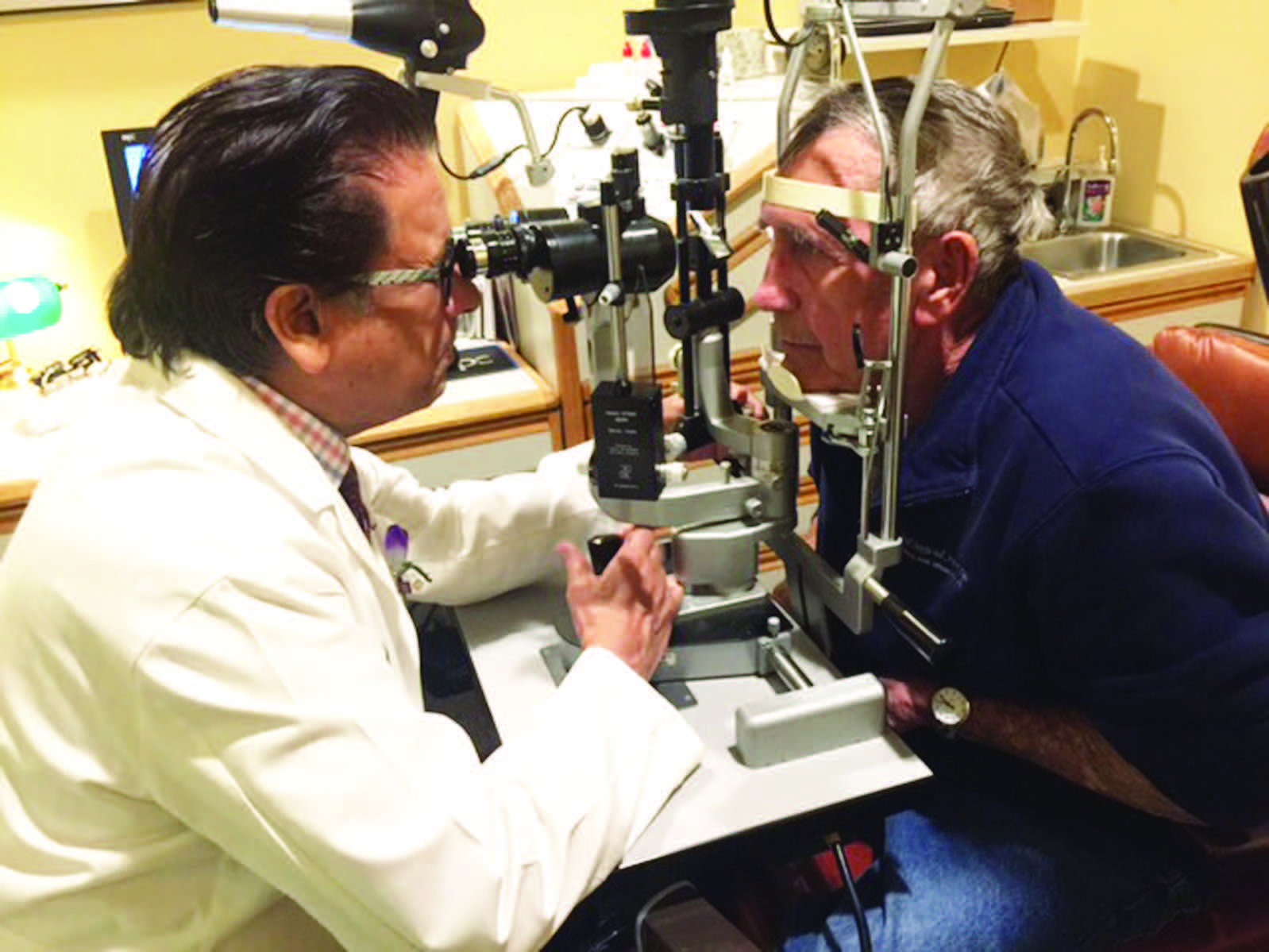 For the past four decades, Dr. Raju and the EFA have been actively and tirelessly on a crusade to eliminate avoidable blindness in areas plagued by poverty and poor access to medical care. The EFA’s mission is to eliminate
For the past four decades, Dr. Raju and the EFA have been actively and tirelessly on a crusade to eliminate avoidable blindness in areas plagued by poverty and poor access to medical care. The EFA’s mission is to eliminate  “I feel so incredibly thankful for my personal and professional gifts, and I make great efforts to share those gifts with those in need of my services,” says Dr. Raju, and he generously gives freely of his own time, money, and medical expertise to help the less fortunate for the past several decades.
“I feel so incredibly thankful for my personal and professional gifts, and I make great efforts to share those gifts with those in need of my services,” says Dr. Raju, and he generously gives freely of his own time, money, and medical expertise to help the less fortunate for the past several decades. The Institute has provided service to more than 400,000 patients and 50,000 surgeries have been performed. It has become an autonomous institution, and Raju has raised over $6 million to establish and fund the two facilities. “You can never be tired of giving back,” he says. “But to have real success, your intentions should be pure. It is a spiritual act.”
The Institute has provided service to more than 400,000 patients and 50,000 surgeries have been performed. It has become an autonomous institution, and Raju has raised over $6 million to establish and fund the two facilities. “You can never be tired of giving back,” he says. “But to have real success, your intentions should be pure. It is a spiritual act.” Dr. Raju hopes that the AAPI joining and collaborating with successful projects such as the Eye Foundation of America’s children’s project will provide continuity of care and the mission of AAPI will be realized, benefitting millions who need eyecare.
Dr. Raju hopes that the AAPI joining and collaborating with successful projects such as the Eye Foundation of America’s children’s project will provide continuity of care and the mission of AAPI will be realized, benefitting millions who need eyecare.




 During his address, Mr. Patnaik applauded the role played by the various organizations involved with the initiative of saving precious lives. Mr. Krishna Kishore Jasthi, Principal Director of Income Tax (Investigation), Odisha, who is the chief coordinator of the project, welcomed the participants, and explained the objectives of the ground-breaking project, “Saving Lives with Bystander CPR” in Odisha.
During his address, Mr. Patnaik applauded the role played by the various organizations involved with the initiative of saving precious lives. Mr. Krishna Kishore Jasthi, Principal Director of Income Tax (Investigation), Odisha, who is the chief coordinator of the project, welcomed the participants, and explained the objectives of the ground-breaking project, “Saving Lives with Bystander CPR” in Odisha. The participants were given a brief presentation of “Heart Disease Among Women” as part of the program by Dr. Pavitra Kotini-Shah, Assistant Professor in the Department of Emergency Medicine, University of Illinois College of Medicine, Chicago, Illinois, USA. Indo-US Faculty team was honored at the conclusion of the program.
The participants were given a brief presentation of “Heart Disease Among Women” as part of the program by Dr. Pavitra Kotini-Shah, Assistant Professor in the Department of Emergency Medicine, University of Illinois College of Medicine, Chicago, Illinois, USA. Indo-US Faculty team was honored at the conclusion of the program. A close friend to the Bush family, he was instrumental in lobbying for the first Diwali celebration in the White House and for President George W. Bush to make his trip to India. He had accompanied President Bill Clinton during his historic visit to India.
A close friend to the Bush family, he was instrumental in lobbying for the first Diwali celebration in the White House and for President George W. Bush to make his trip to India. He had accompanied President Bill Clinton during his historic visit to India.

 “The essence of AAPI is educational,” Dr. Kolli added. “That translates into numerous Continuing Medical Education (CME) and non-CME seminars by experts in their fields. The GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” has had several CME sessions that focused on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, research, and Medical Jeopardy.”
“The essence of AAPI is educational,” Dr. Kolli added. “That translates into numerous Continuing Medical Education (CME) and non-CME seminars by experts in their fields. The GHS 2023 with the theme of “True and Total Health is the Wellbeing of Mind, Body, and Spirit” has had several CME sessions that focused on Mental Health, Infant and Maternal Mortality as well as various other medical specialty updates, research, and Medical Jeopardy.” The second part of the morning session was on Diabetes and Kidney Disease. The scientific presentation on Diabetes Management Update was given by Dr. G.R. Sridhar, while “Diabetic Nephropathy: Current Concepts in Diagnosis” was offered by Dr. Sharma Prabhakar. Dr. K. L. Gupta educated the audience on Lupus Nephritis. “CKD of Unknown Origin & Uddanam Nephropathy” was the theme addressed by Dr. T. Ravi Raju, while “New Insights into the Biology and Mechanism of Renal Fibrosis” was the topic addressed by Dr. Raghu Kalluri. The sessions were moderated by Dr. KAV Subrahmanyam, Dr. K. Dilip Kumar, and Dr. R. K. Sharma.
The second part of the morning session was on Diabetes and Kidney Disease. The scientific presentation on Diabetes Management Update was given by Dr. G.R. Sridhar, while “Diabetic Nephropathy: Current Concepts in Diagnosis” was offered by Dr. Sharma Prabhakar. Dr. K. L. Gupta educated the audience on Lupus Nephritis. “CKD of Unknown Origin & Uddanam Nephropathy” was the theme addressed by Dr. T. Ravi Raju, while “New Insights into the Biology and Mechanism of Renal Fibrosis” was the topic addressed by Dr. Raghu Kalluri. The sessions were moderated by Dr. KAV Subrahmanyam, Dr. K. Dilip Kumar, and Dr. R. K. Sharma. N K Panigrahi opened the session with a brilliant talk on Heart Disease Epidemic, which was followed by an informative session on Heart Failure- What’s New for 2022, presented by Dr. Sreeni Gangasani. Dr. A. Sharath Reddy spoke on Interventional Cardiology Update, and Dr. Brahma Sharma educated the delegates on Current Concepts in Prediction and Prevention of Heart Attacks in South Asians. Structural Heart Disease was the theme of the presentation by Dr. Prasad Chalasani, while Update on Cardiac Surgery was presented by Dr. M. Gopichand.
N K Panigrahi opened the session with a brilliant talk on Heart Disease Epidemic, which was followed by an informative session on Heart Failure- What’s New for 2022, presented by Dr. Sreeni Gangasani. Dr. A. Sharath Reddy spoke on Interventional Cardiology Update, and Dr. Brahma Sharma educated the delegates on Current Concepts in Prediction and Prevention of Heart Attacks in South Asians. Structural Heart Disease was the theme of the presentation by Dr. Prasad Chalasani, while Update on Cardiac Surgery was presented by Dr. M. Gopichand. NATCO Pharma Oncology Session on Sunday, January 8th was chaired by Dr. Satheesh Kathula, Vice President of AAPI, and moderated by Dr. Muralikrishna Voonna and Dr. Sushil Jain. “A focus on newer treatment modalities in Radiation Oncology” was the topic addressed by Dr. Umesh Mahantshetty, while Dr. T. Subramanyeswar Rao spoke about “What’s new in surgical oncology?” An Update on Systemic Therapies for Cancer was provided by Dr. Raghunadharao Digumarti. “Evolving Biology and New Therapies – Strategies to Control Cancer” was the topic addressed by Dr. Raghu Kalluri. An insightful session on Pharmaco economics of cancer drugs – can we afford it?” was presented by Dr. Satheesh Kathula. “India’s unique value proposition towards Medical Tourism” was addressed by Mr. Shaaz Mehmood.
NATCO Pharma Oncology Session on Sunday, January 8th was chaired by Dr. Satheesh Kathula, Vice President of AAPI, and moderated by Dr. Muralikrishna Voonna and Dr. Sushil Jain. “A focus on newer treatment modalities in Radiation Oncology” was the topic addressed by Dr. Umesh Mahantshetty, while Dr. T. Subramanyeswar Rao spoke about “What’s new in surgical oncology?” An Update on Systemic Therapies for Cancer was provided by Dr. Raghunadharao Digumarti. “Evolving Biology and New Therapies – Strategies to Control Cancer” was the topic addressed by Dr. Raghu Kalluri. An insightful session on Pharmaco economics of cancer drugs – can we afford it?” was presented by Dr. Satheesh Kathula. “India’s unique value proposition towards Medical Tourism” was addressed by Mr. Shaaz Mehmood. The much-anticipated Women’s Leadership Forum featured extraordinarily successful Women Leaders representing a diversity of professions, involving public, private and government organizations.
The much-anticipated Women’s Leadership Forum featured extraordinarily successful Women Leaders representing a diversity of professions, involving public, private and government organizations. Medical Education & Research was led by Dr. Lokesh Eadara, Dr. P.V. Sudhakar, and Dr. G. Butchiraju. Community Outreach Program – HPV Vaccination at the Mahatma Gandhi Cancer Hospital, Visakhapatnam was coordinated by Dr. Syed Ahmed, Dr. Murali Krishna Voona, Dr. Meher Bala Medavaram, Secretary of AAPI.
Medical Education & Research was led by Dr. Lokesh Eadara, Dr. P.V. Sudhakar, and Dr. G. Butchiraju. Community Outreach Program – HPV Vaccination at the Mahatma Gandhi Cancer Hospital, Visakhapatnam was coordinated by Dr. Syed Ahmed, Dr. Murali Krishna Voona, Dr. Meher Bala Medavaram, Secretary of AAPI.
 Dr Ravi Kolli, President of AAPI, while describing the objectives of the Summit, said, “The Global Healthcare Summit has served as a means to raising awareness on key health care issues affecting the Indian subcontinent, such as the Stigma of Mental illness, Suicide prevention, Diabetes, Cardiovascular Diseases, Women’s and Children’s Health, Blindness Prevention and Hepatitis etc. Highlight of this Summit was to reaffirm NRI Physicians’ commitment towards improving health care and create model programs for management of various diseases and to improve outcomes universally, he added.
Dr Ravi Kolli, President of AAPI, while describing the objectives of the Summit, said, “The Global Healthcare Summit has served as a means to raising awareness on key health care issues affecting the Indian subcontinent, such as the Stigma of Mental illness, Suicide prevention, Diabetes, Cardiovascular Diseases, Women’s and Children’s Health, Blindness Prevention and Hepatitis etc. Highlight of this Summit was to reaffirm NRI Physicians’ commitment towards improving health care and create model programs for management of various diseases and to improve outcomes universally, he added. In addition, AAPI has plans to collaborate with various state and federal government programs to enhance the quality of healthcare delivery, making it affordable, efficient, and equitable, improving health outcomes universally and training the trainer sessions involving learning modules in different specialties, and tele-consultations.
In addition, AAPI has plans to collaborate with various state and federal government programs to enhance the quality of healthcare delivery, making it affordable, efficient, and equitable, improving health outcomes universally and training the trainer sessions involving learning modules in different specialties, and tele-consultations. Chief Guest at the Summit, Smt. Vidadala Rajini, Honorable Minister for Health, Family Welfare & Medical Education of state of Andhra Pradesh, said, “The Global Healthcare Summit is an important opportunity for all the healthcare professionals to learn from each other and enhance fellowship. I’m grateful to have this opportunity to attend and learn from all of you,” she said. “I believe that by working with you, we can improve the health and wellbeing of the people in the state. The government has the ability to design the best policies on healthcare, while delivering the best treatments and medical care to the patient is essentially in the hands of the physicians.” Among others who addressed the AAPI delegates and joined the felicitation of AAPI delegates and the local organizers of the Summit included, Shri. Gudivada Amarnath, Honorable Minister for IT.
Chief Guest at the Summit, Smt. Vidadala Rajini, Honorable Minister for Health, Family Welfare & Medical Education of state of Andhra Pradesh, said, “The Global Healthcare Summit is an important opportunity for all the healthcare professionals to learn from each other and enhance fellowship. I’m grateful to have this opportunity to attend and learn from all of you,” she said. “I believe that by working with you, we can improve the health and wellbeing of the people in the state. The government has the ability to design the best policies on healthcare, while delivering the best treatments and medical care to the patient is essentially in the hands of the physicians.” Among others who addressed the AAPI delegates and joined the felicitation of AAPI delegates and the local organizers of the Summit included, Shri. Gudivada Amarnath, Honorable Minister for IT. Describing some of the objectives of the GHS, Dr. Prasad Chalasani, Chair of GHS (USA) 2023 said. “We have tried to create an intellectually charged platform for experts to share their knowledge and experiences on some of the common professional issues that remain a challenge in spite of all the advances. The exchange of expertise and transfer of technology by the best brains is bound to offer positive and innovative solutions to some of the problems faced by humankind.”
Describing some of the objectives of the GHS, Dr. Prasad Chalasani, Chair of GHS (USA) 2023 said. “We have tried to create an intellectually charged platform for experts to share their knowledge and experiences on some of the common professional issues that remain a challenge in spite of all the advances. The exchange of expertise and transfer of technology by the best brains is bound to offer positive and innovative solutions to some of the problems faced by humankind.” AAPI, in collaboration with the AAPI India Foundation administered free HPV vaccines to over 100 low income young women from several government schools in the region, during a special launch and awareness camp organized at the Mahatma Gandhi Cancer Hospital, Visakhapatnam in India on Saturday, January 7th, 2023 with the objective of creating awareness and preventing cervical cancer, a leading cause of cancer deaths among women in India.
AAPI, in collaboration with the AAPI India Foundation administered free HPV vaccines to over 100 low income young women from several government schools in the region, during a special launch and awareness camp organized at the Mahatma Gandhi Cancer Hospital, Visakhapatnam in India on Saturday, January 7th, 2023 with the objective of creating awareness and preventing cervical cancer, a leading cause of cancer deaths among women in India. Dr. Udaya Shivangi, Chair of AAPI’s Women’s Committee, in her opening remarks provided an overview of the Forum and the many initiatives by the Forum both in India and the United States. Shri. MVV Satyavathi, Member of Parliament, representing Anakapalli was the Guest of Honor at the Women’s Forum. In her address, she congratulated AAPI, whose members having been born and educated in India, settled down in the US with success, have come back to India to serve the people of India and work together for the betterment of humanity.
Dr. Udaya Shivangi, Chair of AAPI’s Women’s Committee, in her opening remarks provided an overview of the Forum and the many initiatives by the Forum both in India and the United States. Shri. MVV Satyavathi, Member of Parliament, representing Anakapalli was the Guest of Honor at the Women’s Forum. In her address, she congratulated AAPI, whose members having been born and educated in India, settled down in the US with success, have come back to India to serve the people of India and work together for the betterment of humanity. The women leaders of AAPI dazzled on stage with elegance, and showcasing their talents by presenting two amazing Fashion Shows on Friday and Saturday at the Summit to the delight of the AAPI delegates.
The women leaders of AAPI dazzled on stage with elegance, and showcasing their talents by presenting two amazing Fashion Shows on Friday and Saturday at the Summit to the delight of the AAPI delegates.